Module 4: Principles and Application of Tactical Field Care (TFC)
Joint Trauma System
Principles and Application of Tactical Field Care (TFC)
The Curriculum Change Log serves as a centralized reference to quickly track recent updates to training materials. It supports trainers by promoting clear communication, accountability, and alignment, helping stakeholders and learners understand what changes were made, why they were implemented, and when they occurred.
As a Combat Medic/Corpsman you are the first medical provider to care for the casualty and initiate more advanced treatments. As such, it is important that you understand the roles and responsibilities of the nonmedical personnel (ASM and CLS) that may be providing care/assisting in care in the prehospital environment.
There are five cognitive and two performance learning objectives for the Principles and Application of Tactical Field Care module. The cognitive learning objectives are:
- Identify the importance of security and safety.
- Identify the basic principles of removal/extraction of casualties from a unit-specific platform.
- Identify the importance of and techniques for communicating casualty information with unit leadership and/or other medical personnel.
- Identify the relevant tactical and casualty data for communicating casualty information.
- Identify triage considerations in Tactical Field Care.
The performance learning objectives are:
- Demonstrate communication of casualty information to tactical leadership and/or other medical personnel.
- Demonstrate the consolidation and triage of casualties at a casualty collection point.
Tactical Field Care is the second of three phases of Tactical Combat Casualty Care. It is the care provided once the responder and casualty are no longer under direct threat from effective enemy fire.
This allows for the time and the relative safety for a more deliberate approach to casualty assessment and treatment.
Keep in mind that the duration of the TFC phase of care could vary from minutes to hours depending on the tactical situation and the availability of evacuation assets.
CASUALTY COLLECTION POINT OVERVIEW (VIDEO)
Tactical Field Care, or TFC, is the care rendered by the first responder, Combat Lifesaver, and/or Combat Medic/Corpsman (CMC) and there is no longer a direct threat or under effective enemy fire. TFC also encompasses care in the combat/tactical environment not involving enemy fire, such as a parachute injury or vehicle crash.
The TFC environment allows the time and relative safety for the medic to assess and treat casualties more deliberately following the MARCH PAWS algorithm. Keep in mind that the tactical situation could revert to care under fire at any time.
Although extraction scenarios will vary based on unit, mission, and vehicle types, a couple of principles apply universally.
SAFETY
The first principle is safety. Avoid additional casualties during any attempts at extraction. Extraction scenarios present many hazards, including fire, smoke, secondary explosions, instability of damaged vehicles or buildings, etc.
MARCH
The second principle is to remember that the MARCH treatment priorities still apply and do not change because the casualty scenario requires extraction. If lifesaving treatments like tourniquet application can be done before completing the extraction, they should be done and monitored during the extraction process. If the casualty is in a position where access to provide immediate lifesaving treatments can’t be accomplished, then they need to be extracted as quickly as is safely possible.
TRAINING
The third principle is training. It is important for both medical and nonmedical personnel to gain and maintain proficiency in extraction of casualties from unit-specific vehicles through training before and during deployments. The time to learn and establish battle drills is before deployment and before the mission.
The CMC should always be ready to receive casualties in an area that provides adequate cover so that lifesaving interventions can be performed. If possible, communicate with the first responder and casualty about the MOI and what treatment has been rendered.
Always reassess lifesaving interventions that were conducted in CUF or TFC using the MARCH PAWS algorithm. If a first responder is available, direct them to assist with exposing and treating the casualty. First responders can also help to prepare medical equipment, pre-stage litters, and document basic information.
Ensure that you document all findings and treatments on a DD Form 1380 TCCC Casualty Card and attach it to the casualty.
Establish a security perimeter in accordance with unit standard operating procedures and/or battle drills.
The tactical situation is fluid and can change quickly. Maintain tactical situational awareness and be aware of your surroundings.
Casualties with altered mental status (shock, head injuries, narcotics, etc.) should immediately be disarmed of weapons, communications equipment, and/or other sensitive items. The items should then be secured by their unit point of contact (POC), taking responsibility for it.
In TFC, available medical equipment is still limited to that carried on the mission by the casualty (their JFAK), other first responders/CLSs (JFAK or unit combat lifesaver bag), and/or a responding CMC (aid bag, etc.). Remember, whenever possible, use the casualty’s JFAK supplies first.
As the tactical situation can change unexpectedly, the first responders and combat medics should be prepared to move with their casualties and equipment on short notice if needed.
In the Tactical Field Care phase, the MARCH PAWS algorithm is followed for a more deliberate approach to the assessment and treatment of casualties than was possible during Care Under Fire.
A full tactical trauma assessment should follow the MARCH PAWS sequence.
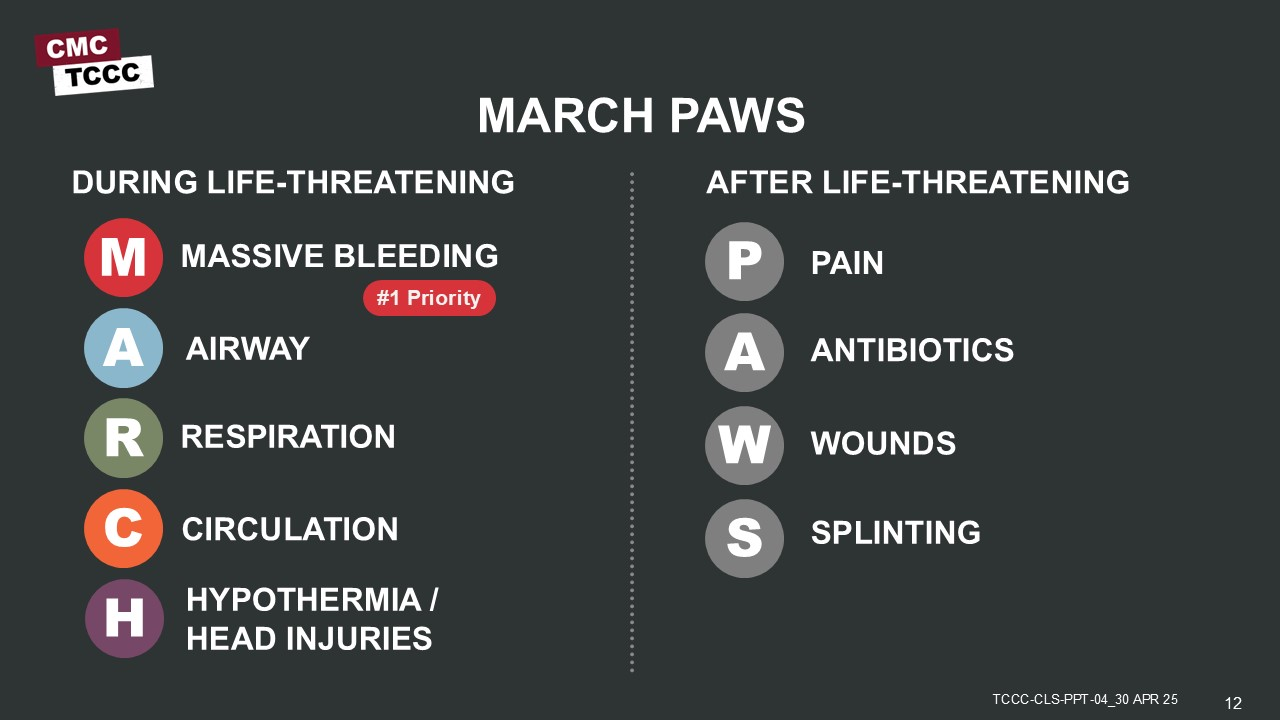
MARCH
- Massive bleeding
- Airway
- Respiration/breathing
- Circulation
- Hypothermia/Head injuries
PAWS
- Pain
- Antibiotics
- Wounds
- Splinting
The specifics of assessment and treatment performed by the Combat Medic/Corpsman in each step of the MARCH PAWS sequence will be discussed in subsequent modules.
The Combat Medic/Corpsmen (CMC) will continuously communicate with the casualty (if possible) by encouraging, reassuring, and explaining each step of care being rendered. Being wounded can cause significant anxiety and fear above and beyond the psychological trauma of combat. Talking frankly with the casualty about their injuries and offering reassurance by describing the treatments being rendered and emphasizing that everything possible is being done to care for them can help decrease their anxiety.
Be honest about the injuries sustained but maintain a positive attitude about treatment and timely evacuation. Talking with the casualty helps assess their mental status, while talking through procedures helps maintain your own focus and confidence as well as the casualty’s confidence in you.
Communicate with first responders, other medical personnel, and tactical leadership about casualty injuries, condition, movement, status, and ongoing care (including annotating treatment on DD Form 1380).
Communicate with tactical leadership immediately on evacuation requirements and throughout casualty treatment. Tactical leadership needs to understand the potential impact to the mission. Unit tactical standard operating procedures and/or battle drills will determine who will communicate with the evacuation system including the 9-line MEDEVAC requests and MIST report(s) (complete review of the 9-line MEDEVAC request and MIST report covered in Module 21). It is up to the CMC to help teach and supply information that is required for evacuation requests and reports.
The CMC will continue treatment until handoff to a higher or equal level of care.
Example of what information the tactical leadership may need to know:
- How many casualties?
- What is the casualty's initial evacuation category?
- Who was injured (key leader/personnel)?
- Can the casualty still fight (ambulatory vs. litter)?
- Urgency of evacuation?
Unit tactical standard operating procedures and/or battle drills determine who communicates with evacuation assets (the medical evacuation coordination cell) to coordinate for TACEVAC/MEDEVAC and with responding medical personnel. This includes 9-line MEDEVAC requests and MIST reports, including:
- Number of casualties
- Injuries that were sustained
- Status of each casualty
- Treatments rendered and treatments needed
- Medical or evacuation equipment requirements
Document and update all casualty assessment and treatment (including interventions and medications) on the DD Form 1380 and communicate these findings during the hand-off to receiving medical and/or evacuation personnel.
Triage is the deliberate sorting of casualties and allocation of limited treatment resources according to a system of priorities designed to maximize the number of survivors on the battlefield. The tenet of triage is doing the greatest good for the greatest amount of people.
When there are multiple casualties, the CMC may need to triage casualties into prioritized treatment groups (immediate, delayed, minimal, expectant) based upon severity of injuries before providing care or assisting other first responders, combat lifesavers, and medical personnel with casualty care.
The CMC will typically care for the most urgent casualties, while other first responders assist, care for less urgent casualties, monitor casualties after emergency interventions, and help prepare casualties for evacuation.
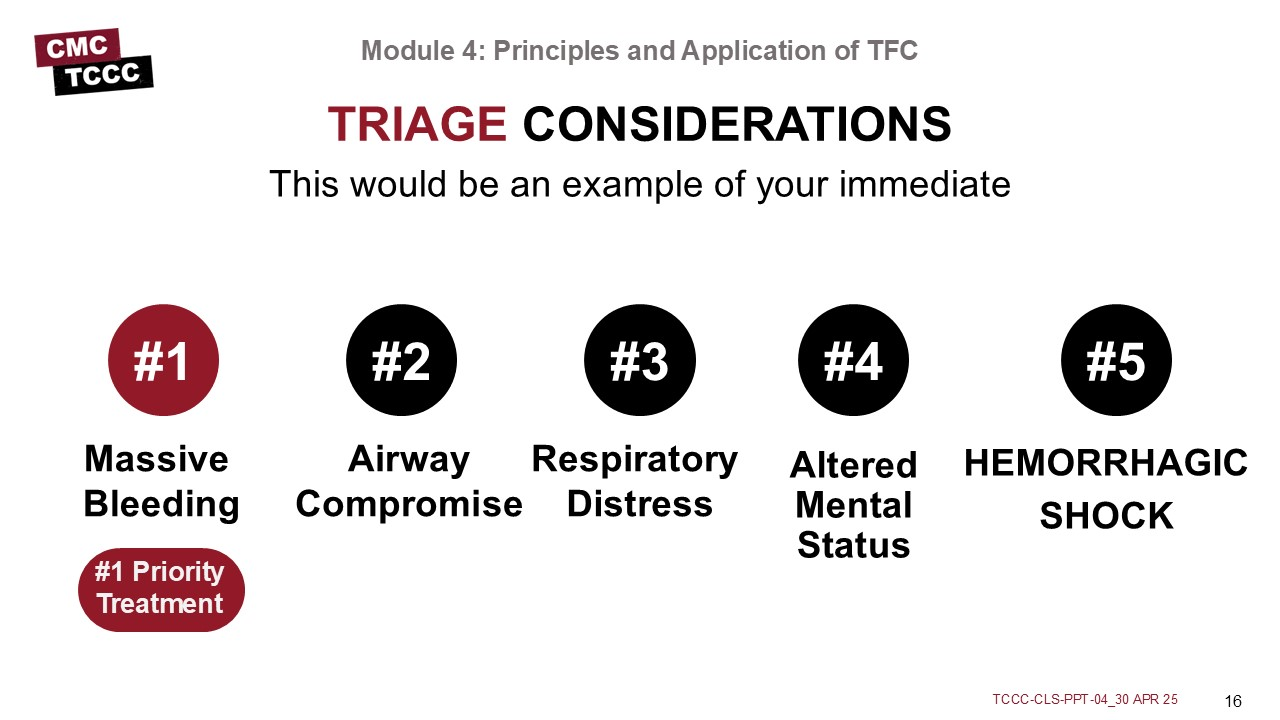
The Combat Medic/Corpsman should consider these priorities (which follow the MARCH sequence) in deciding how to prioritize treatment/evacuation of multiple casualties in the TFC phase of care. This can be challenging, especially when casualties are known to the medic (in the same unit, for example).
It is particularly important not to expend limited resources (time, medical equipment and supplies, etc.) on a casualty who is not expected to reach a higher level of medical care alive, as this could compromise the treatment of higher-priority patients. Expectant casualties should not be abandoned but should be treated with remaining time and resources after immediate and delayed patients have been treated.
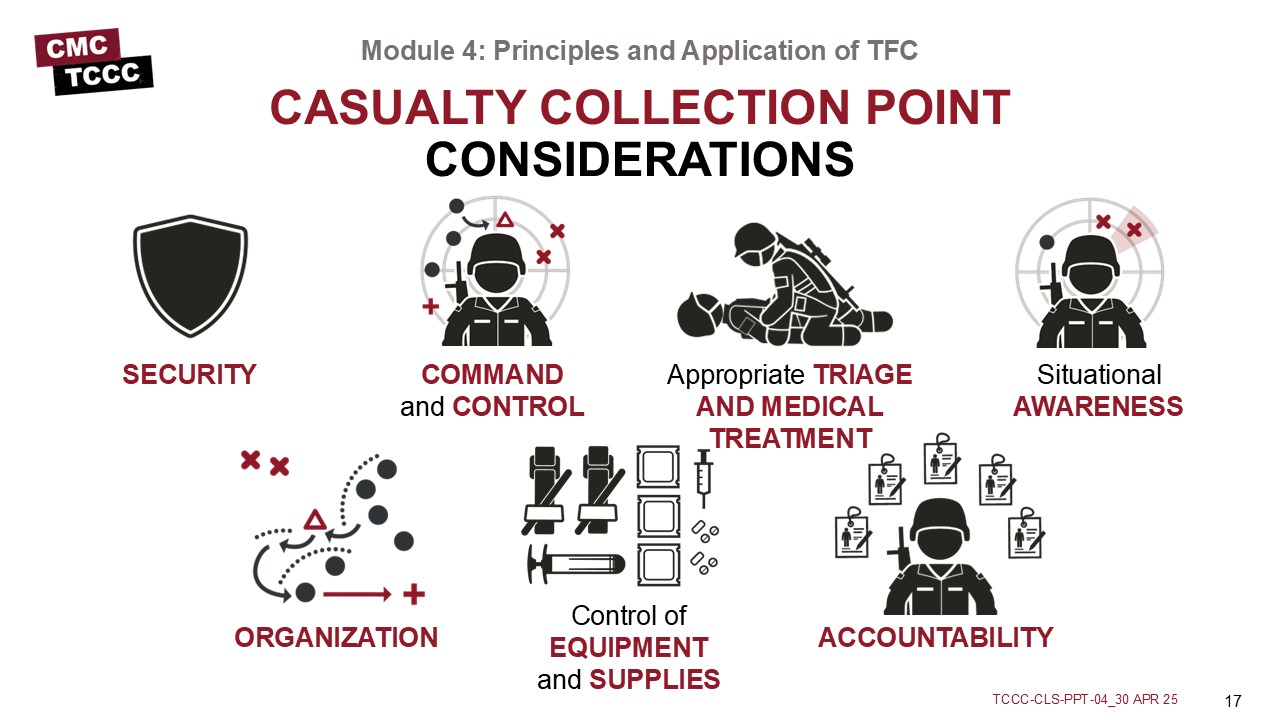
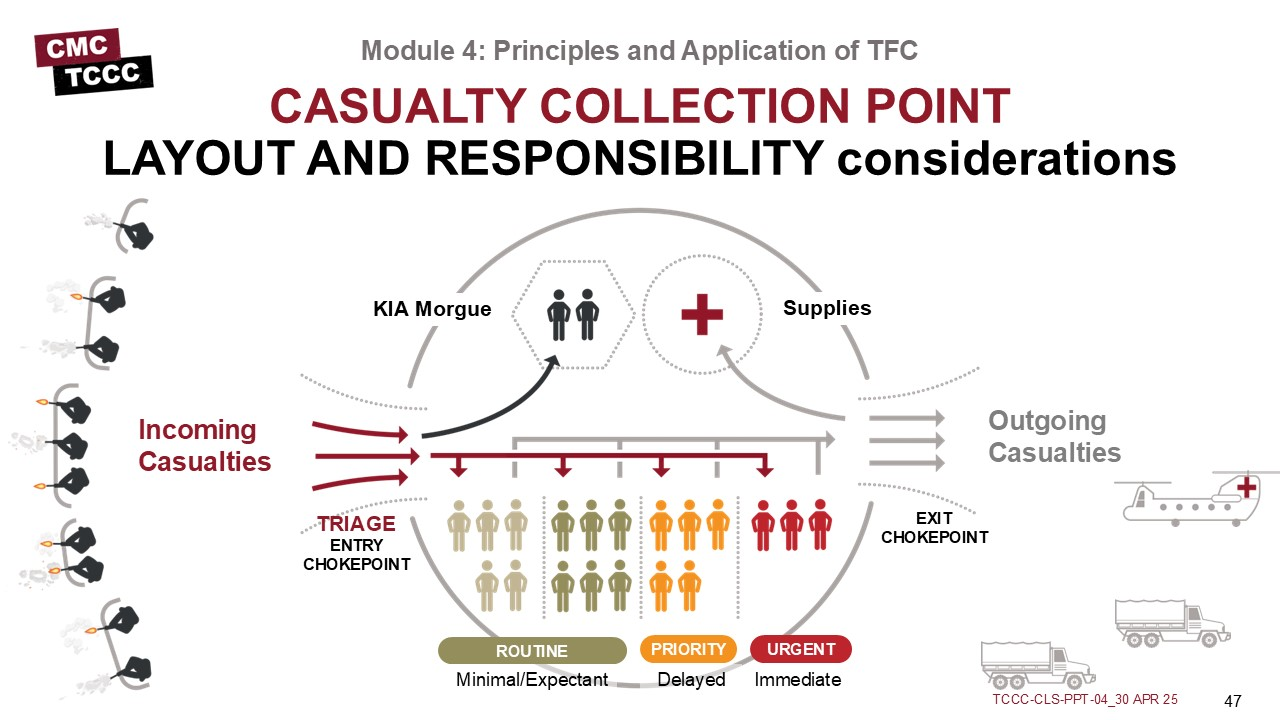
The following are key considerations for unit leadership and medical personnel in planning, establishing, and operating a tactical CCP in support of combat operations:
- Maintain security Maintain command and control
- Maintain appropriate triage and medical treatment protocols
- Maintain situational awareness
- Maintain organization
- Maintain control of medical equipment and supplies
- Maintain accountability of personnel and casualties
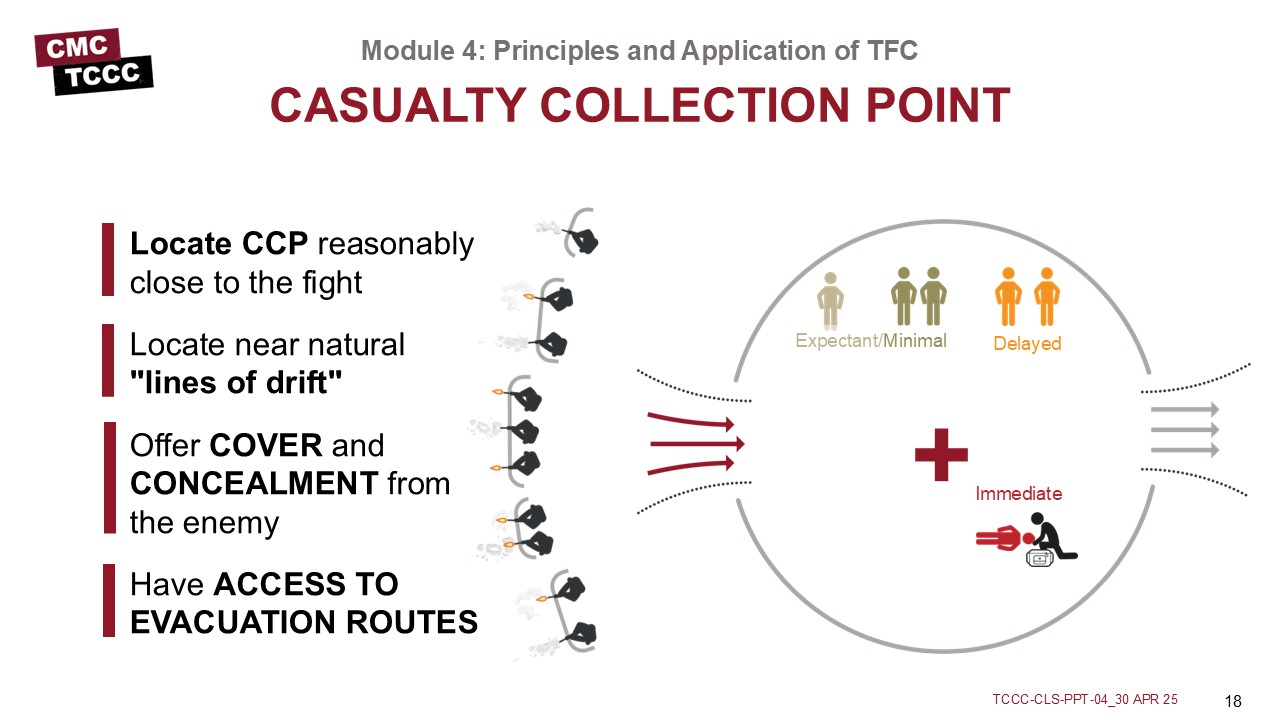
Tactical Casualty Collection Points (CCPs) should be established reasonably close to the fight where casualties are likely to occur, be near natural “lines of drift,” provide relative cover and concealment from the enemy whenever possible and have access to evacuation routes.
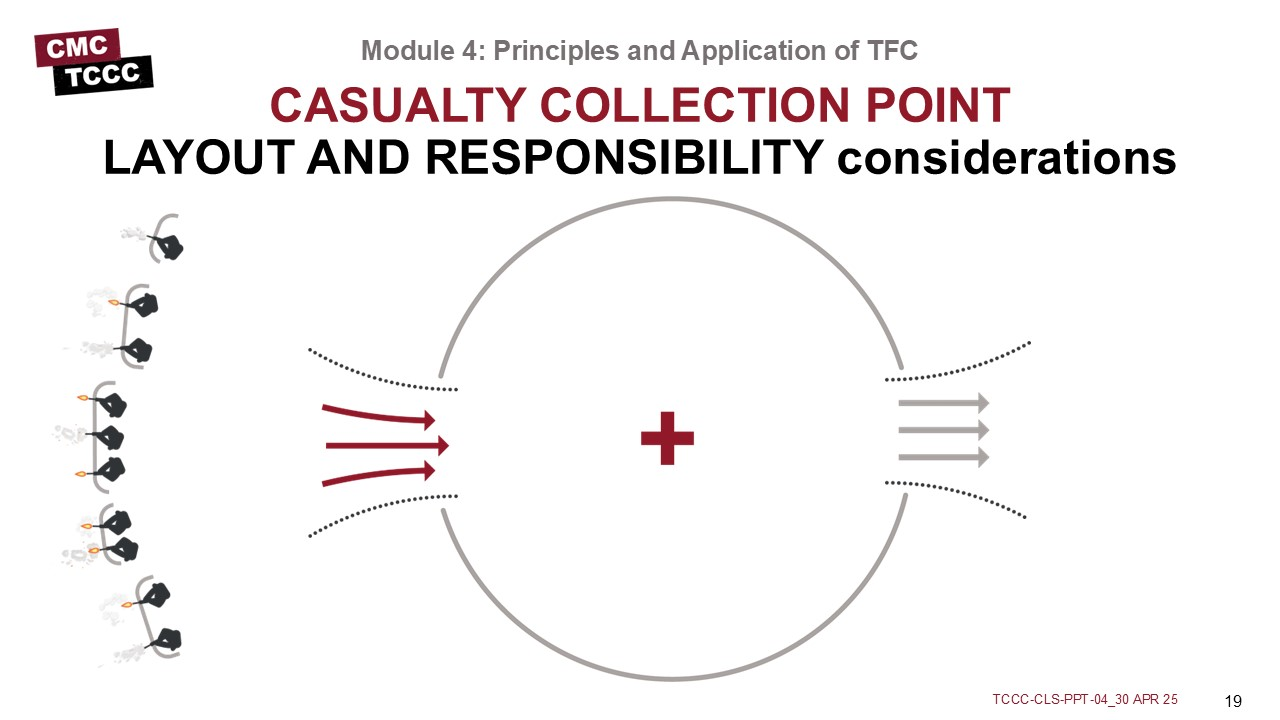
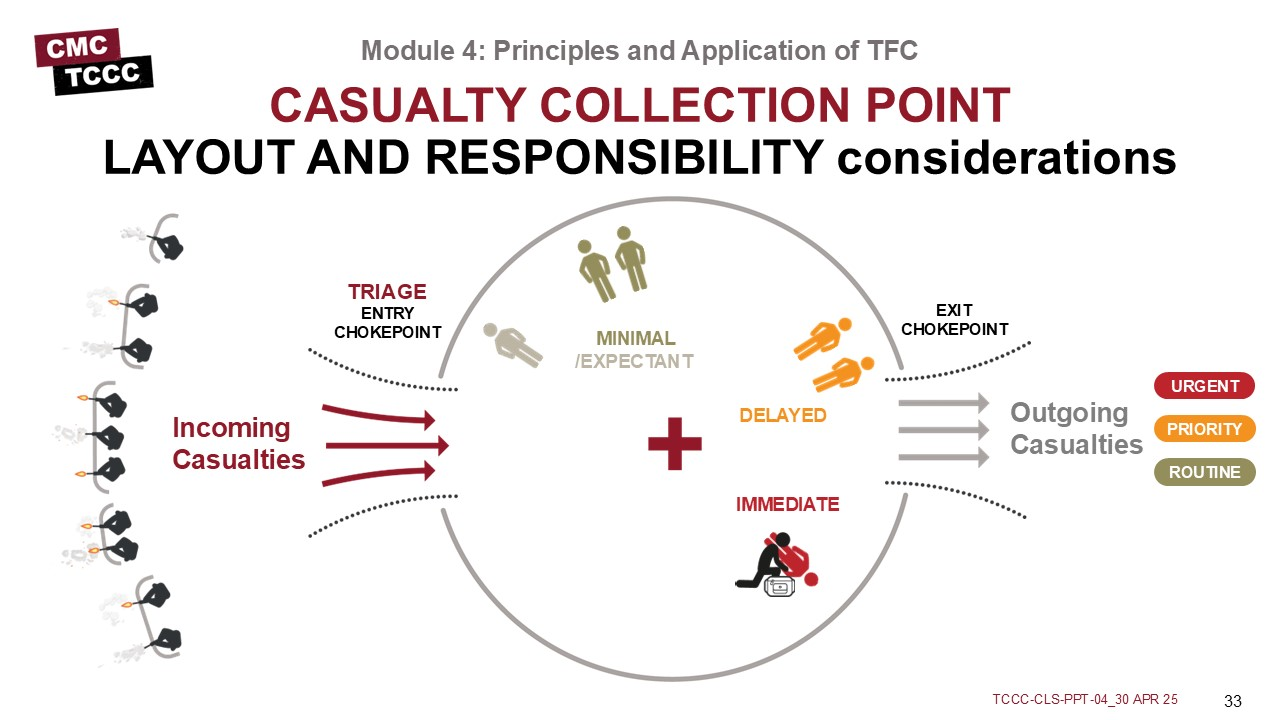
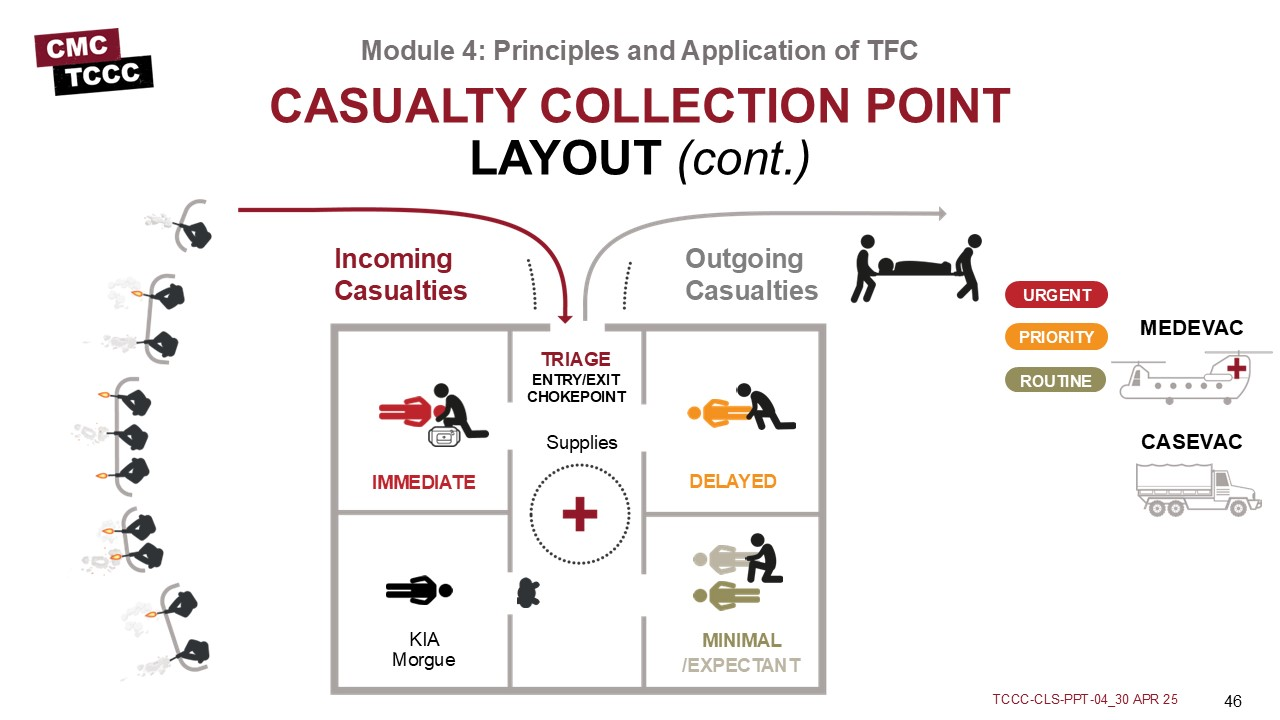
Medical personnel are responsible for everything inside the CCP, including triage, casualty treatment and monitoring, packaging and staging casualties for evacuation, requesting assistance as needed from other unit assets, providing guidance and recommendations to leadership on casualty management and evacuation, medical equipment and supplies.
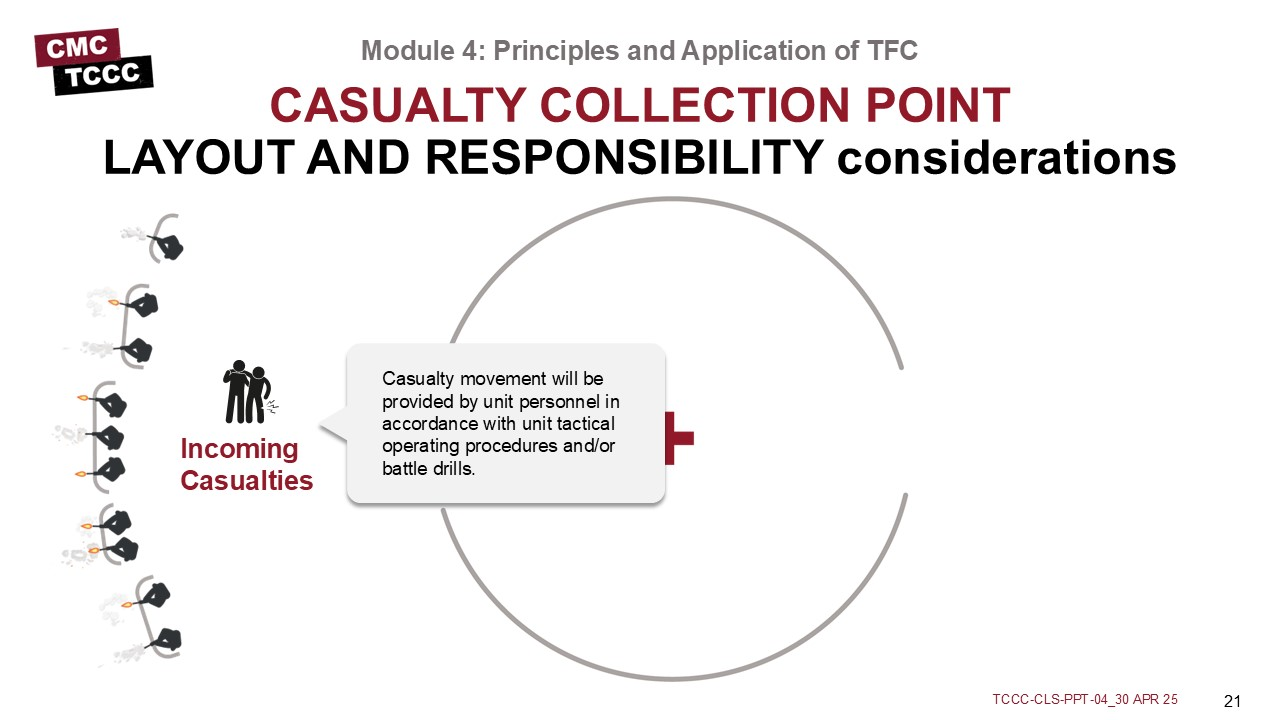
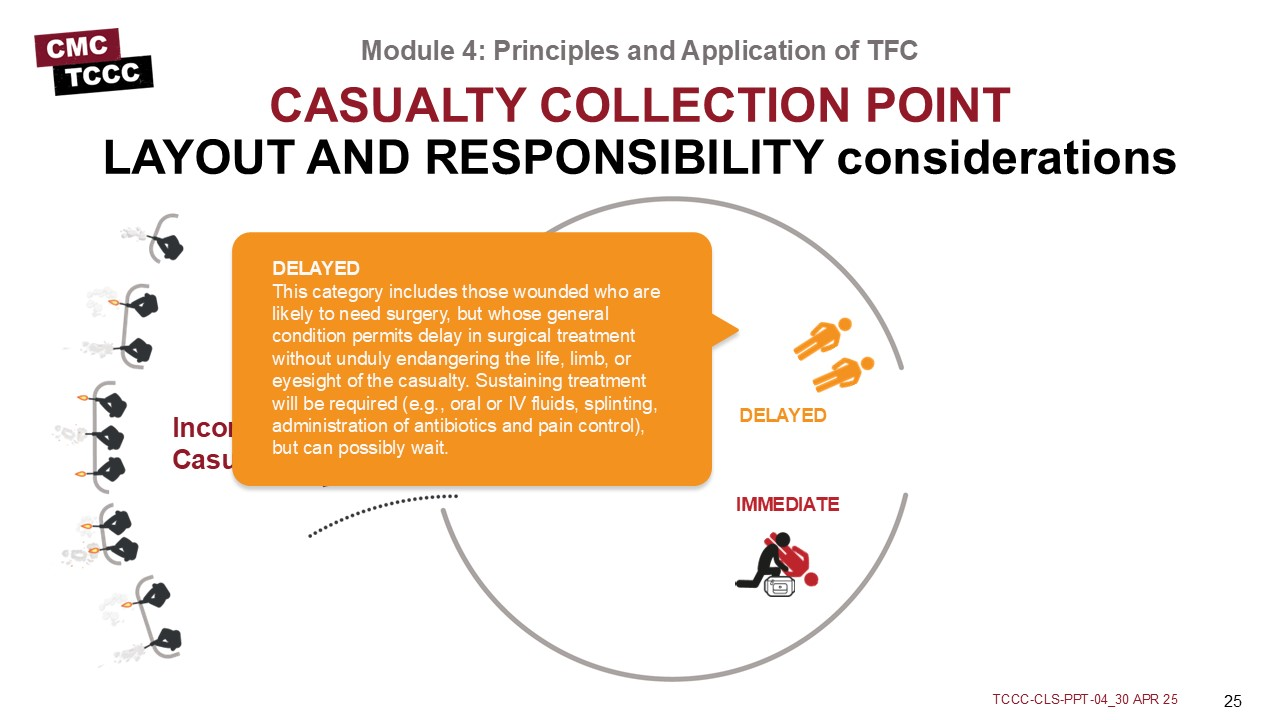
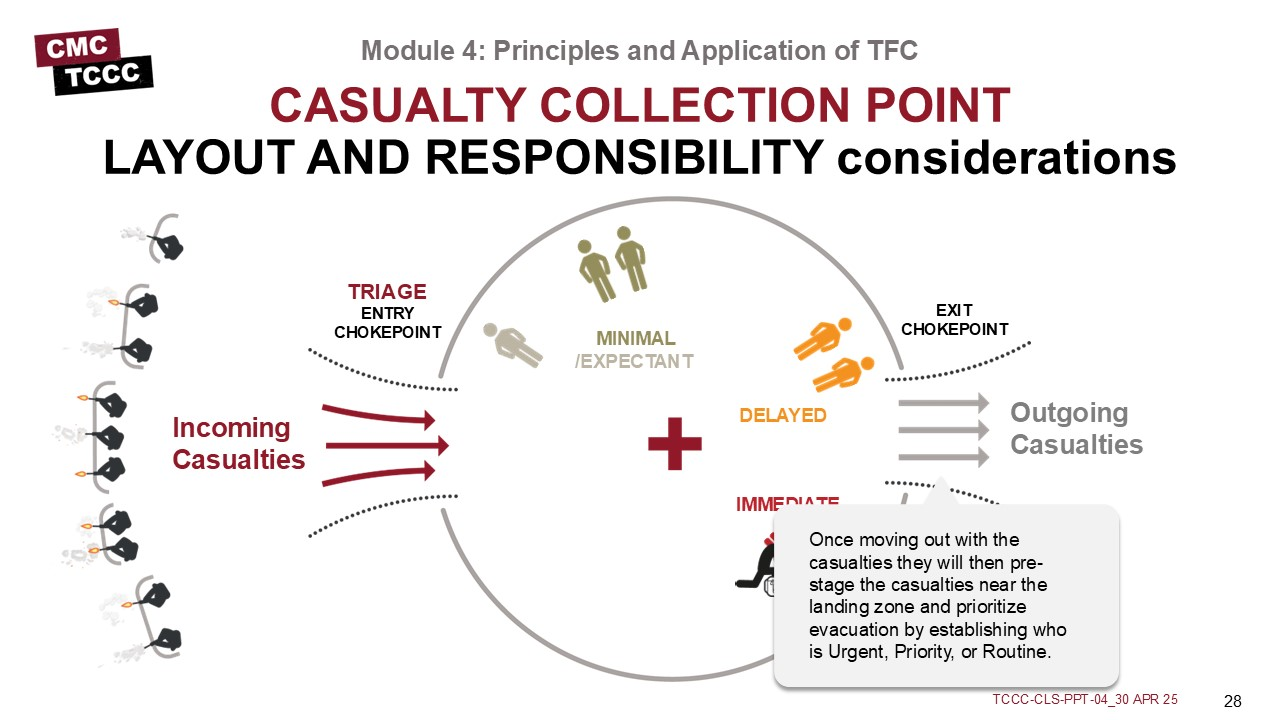
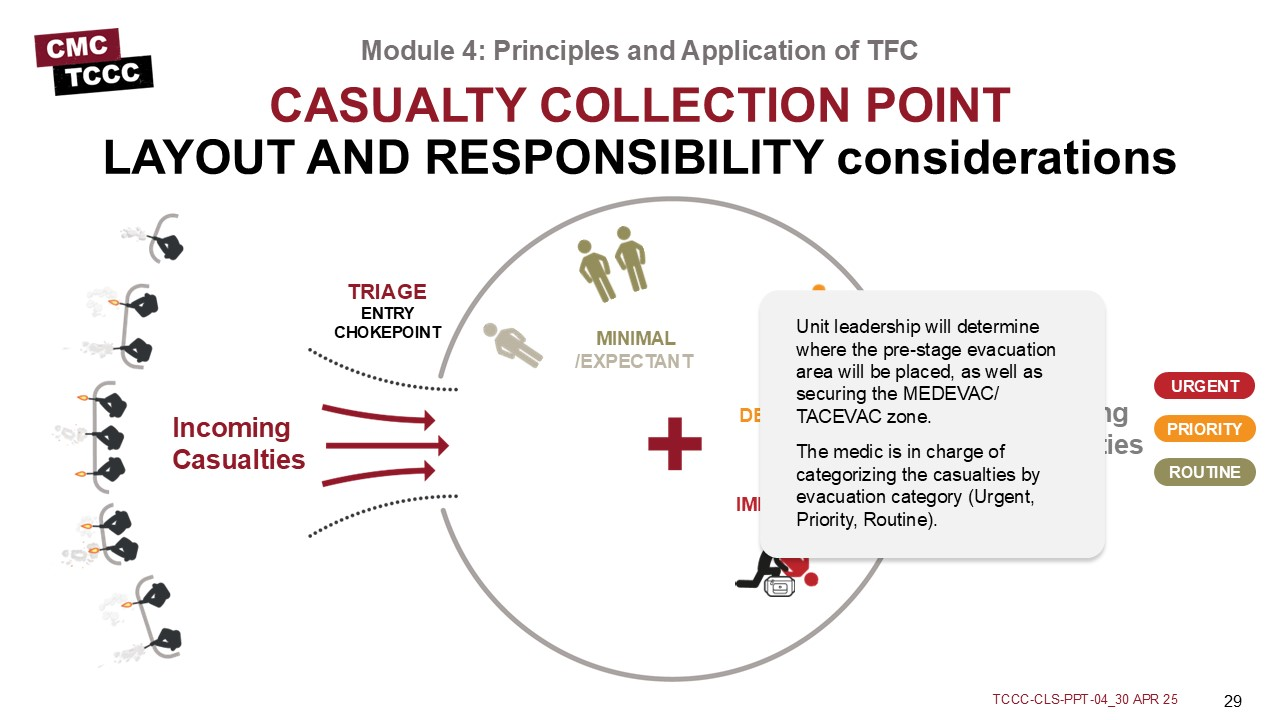
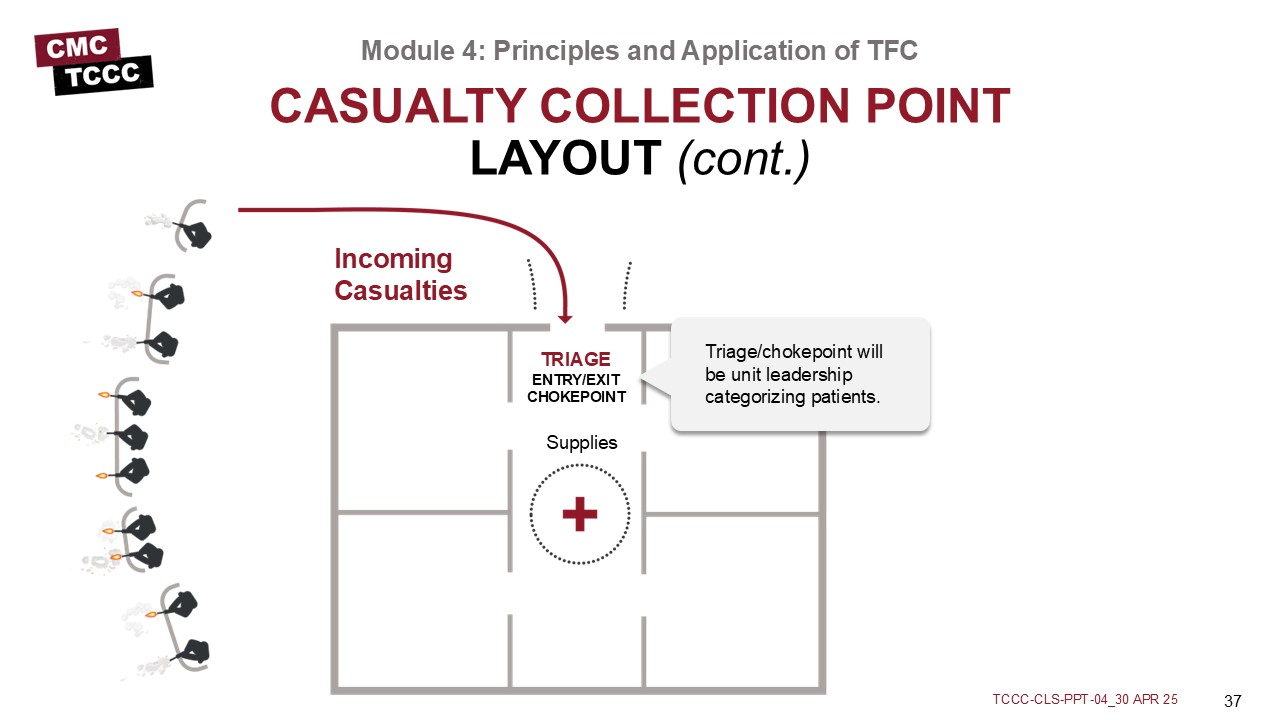
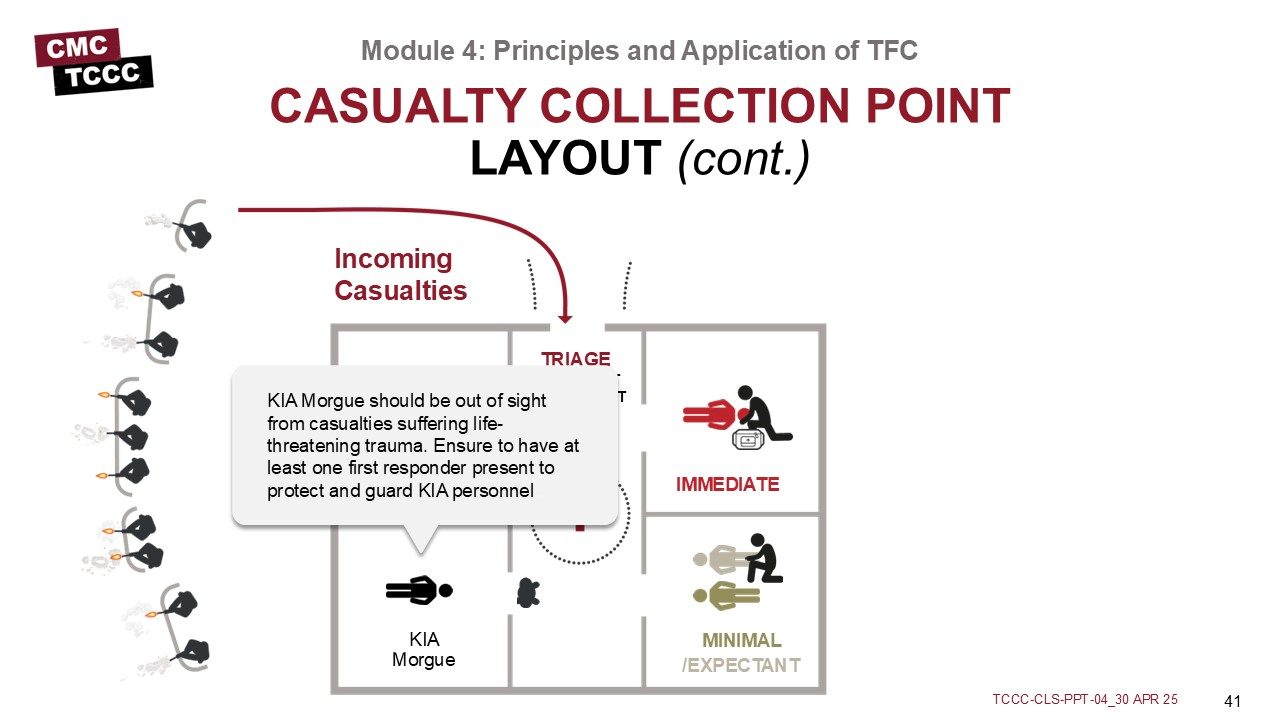
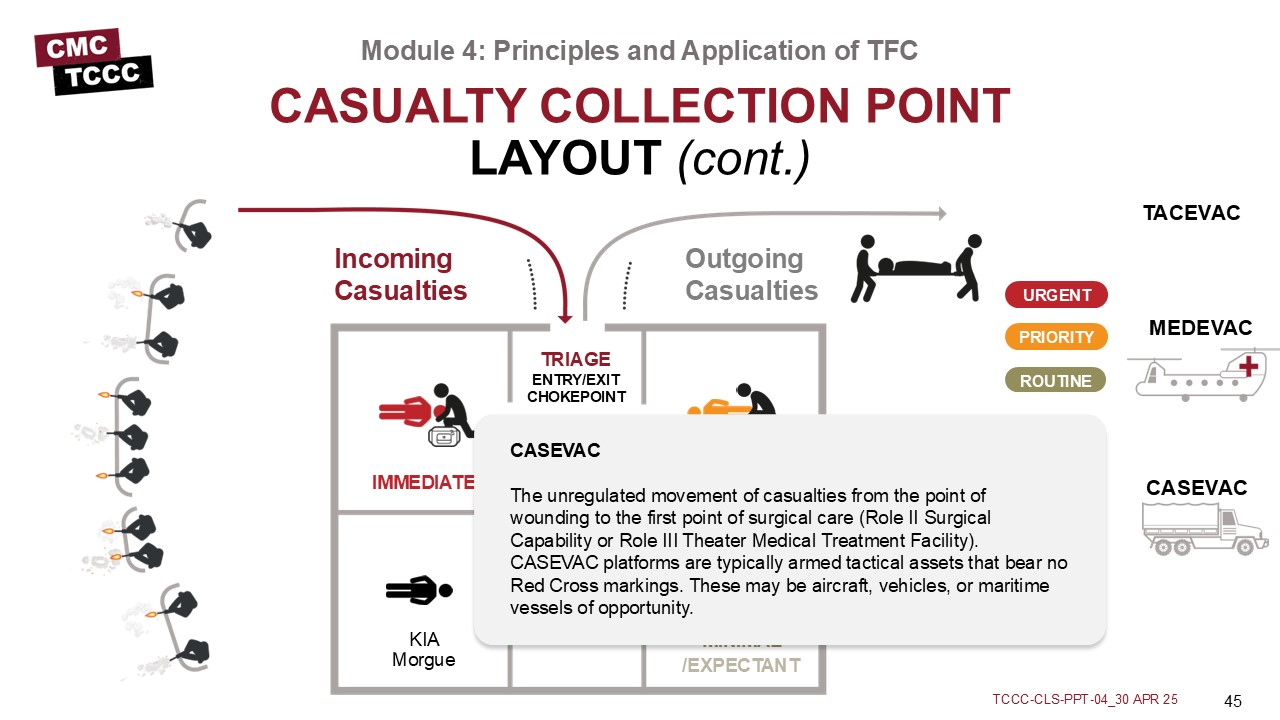
In an ideal layout, there are separate entry and exit points (which are potential chokepoints) to control casualty flow through the CCP, similar to what is seen in this example.
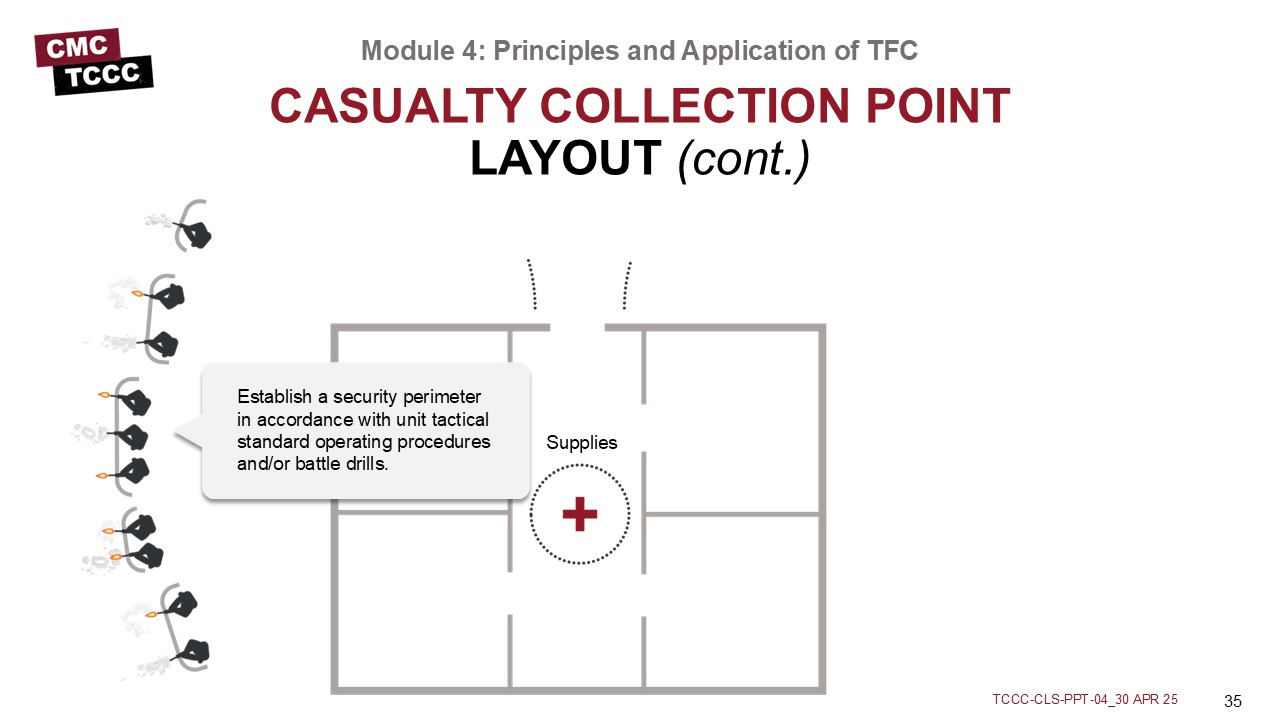
Establish a security perimeter in accordance with unit tactical standard operating procedures and/or battle drills.
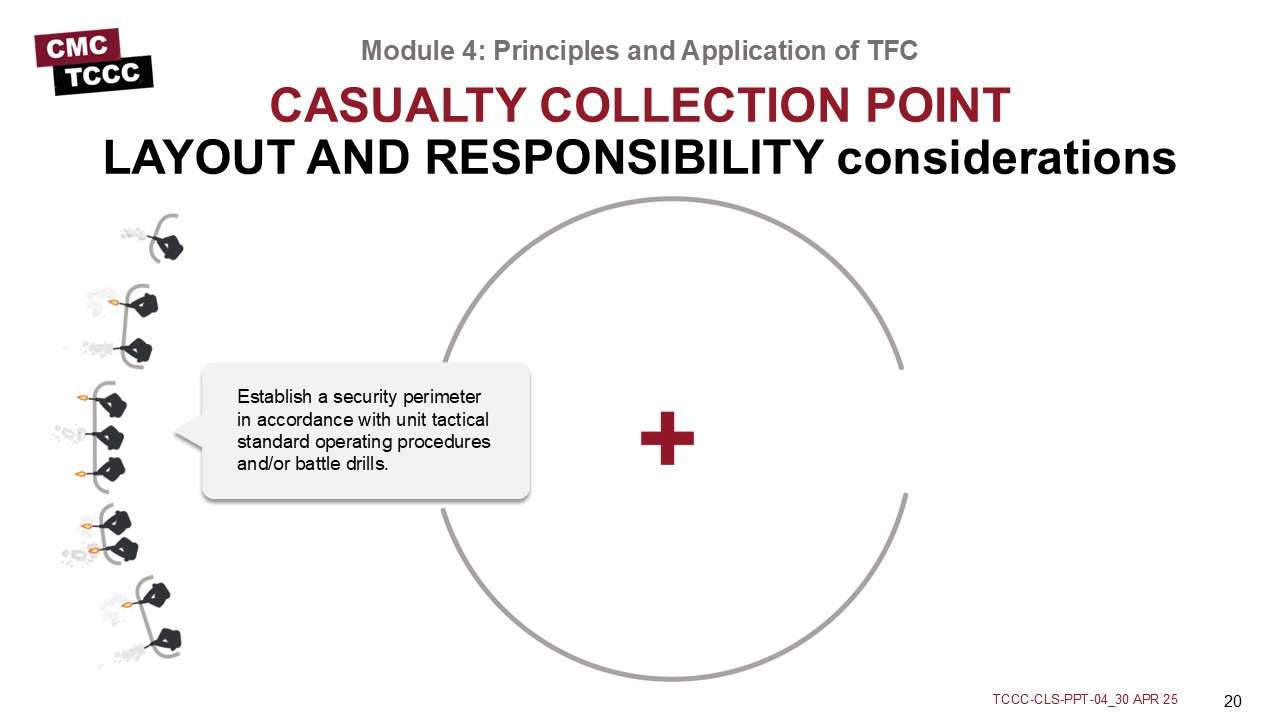
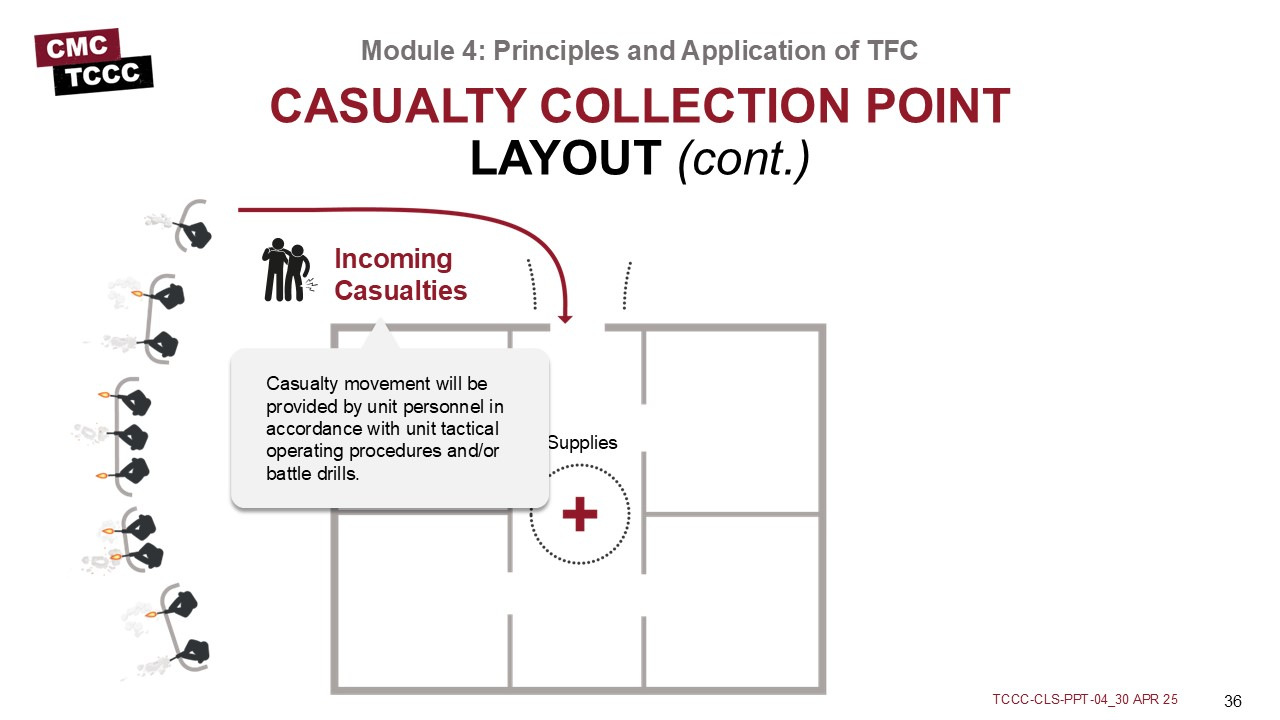
Casualty movement will be provided by unit personnel in accordance with unit tactical operating procedures and/or battle drills.
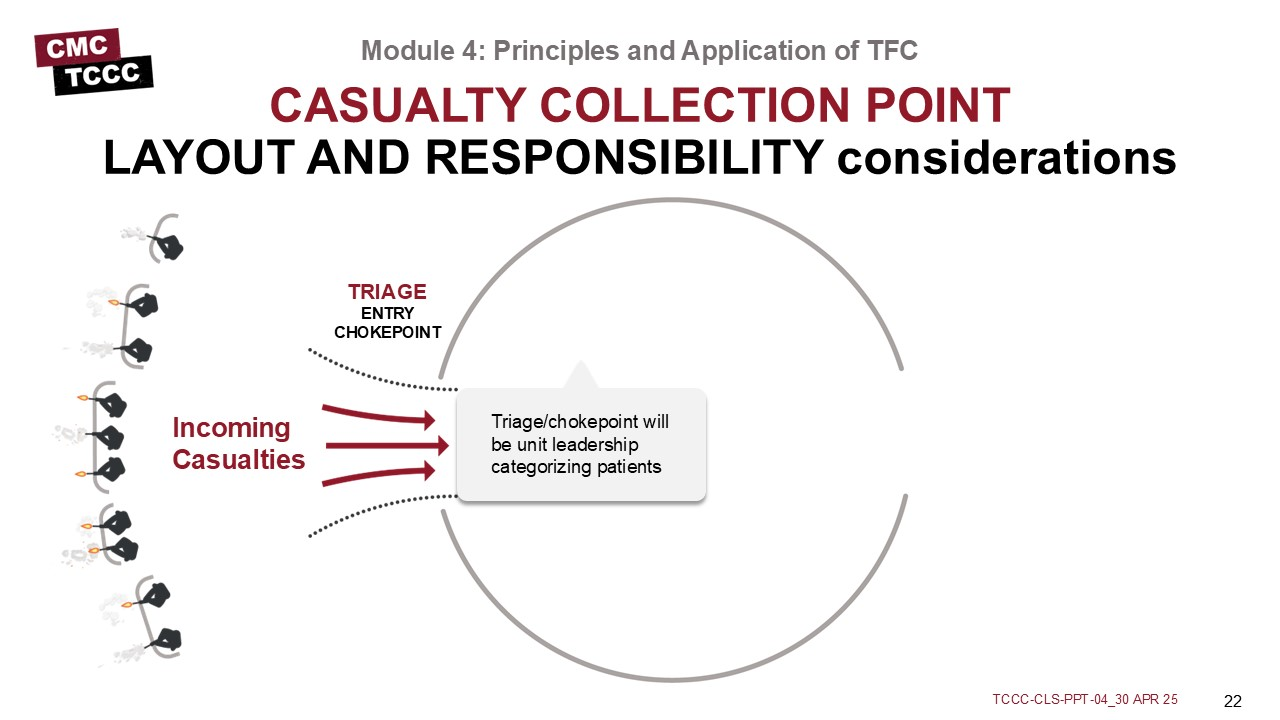
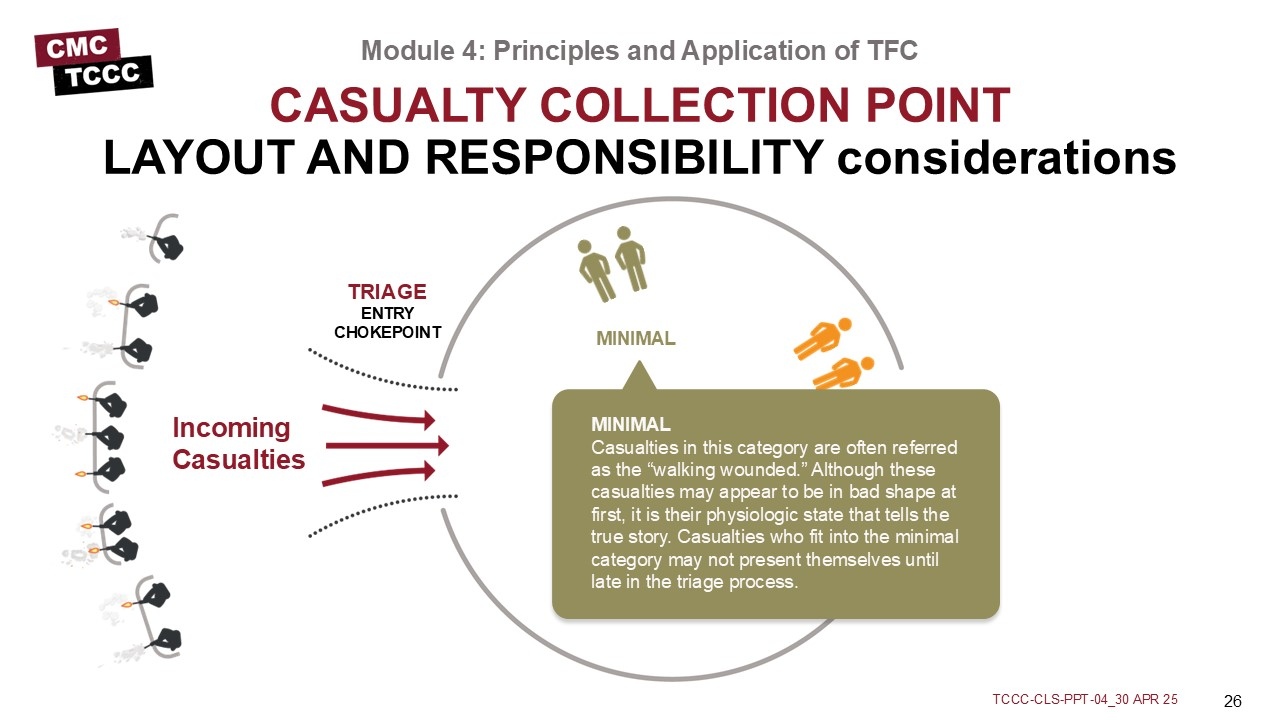
Triage/chokepoint will be unit leadership categorizing patients
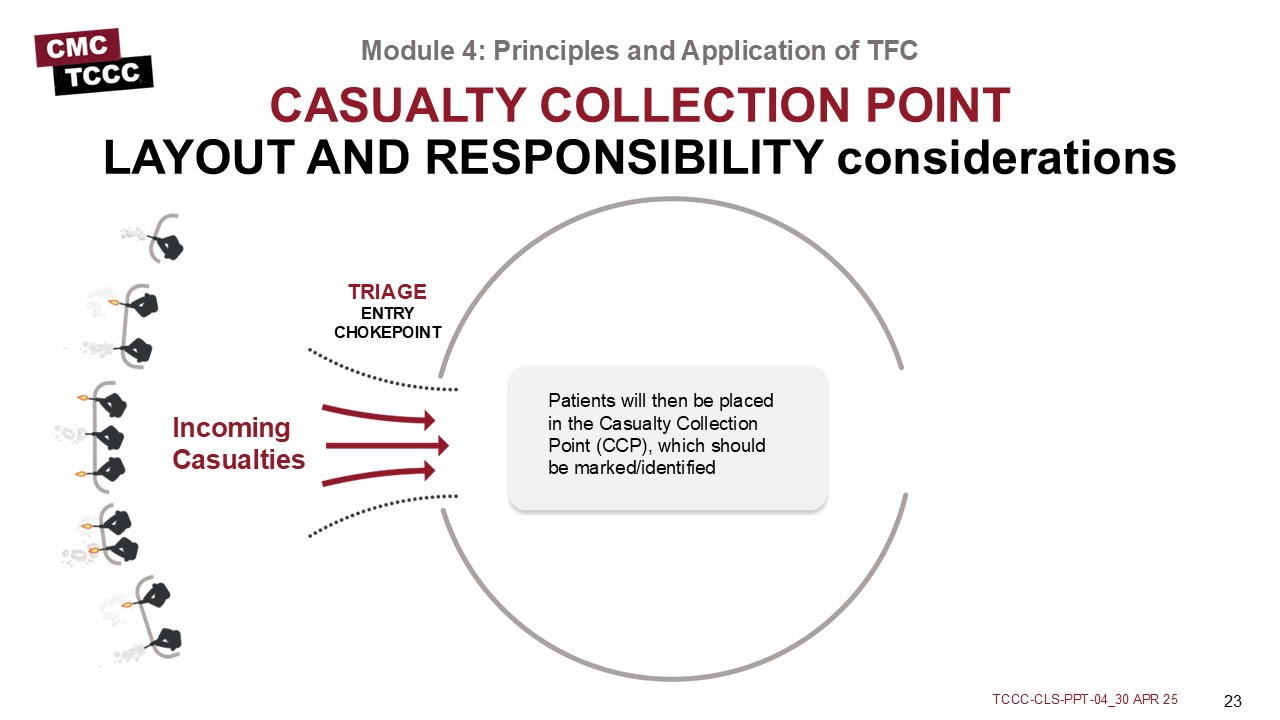
Patients will then be placed in the Casualty Collection Point (CCP), which should be marked/identified
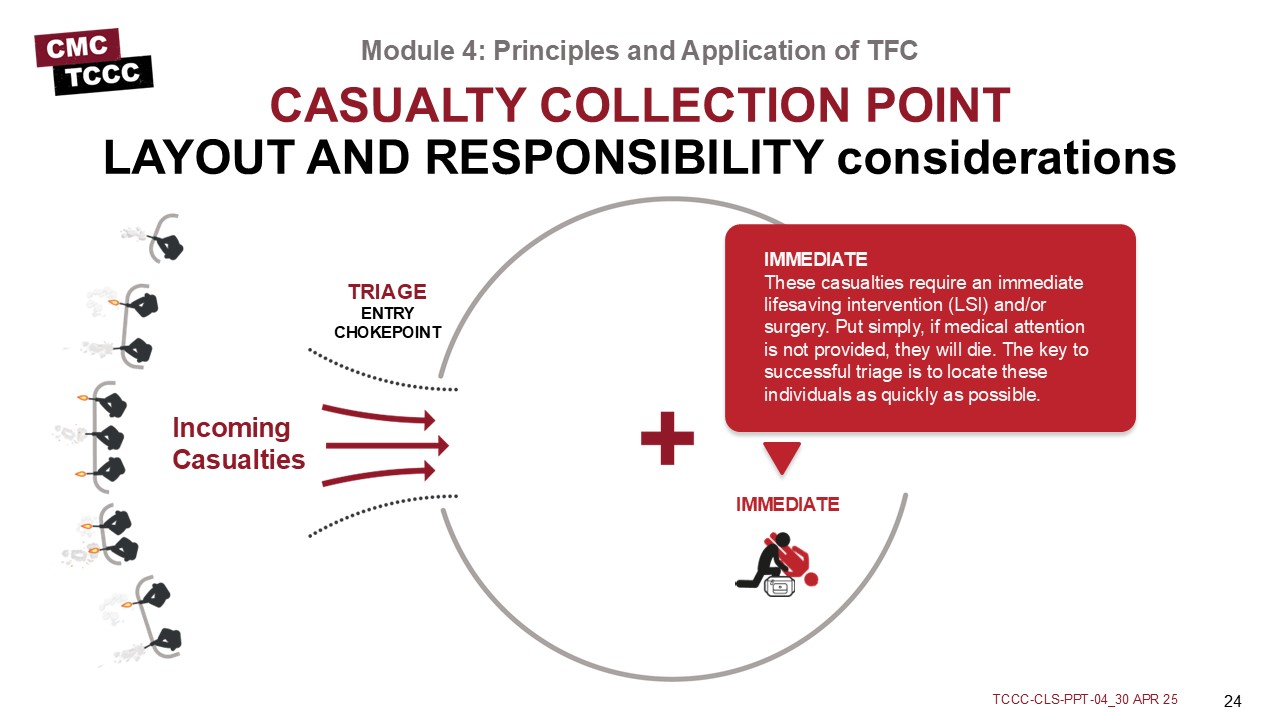
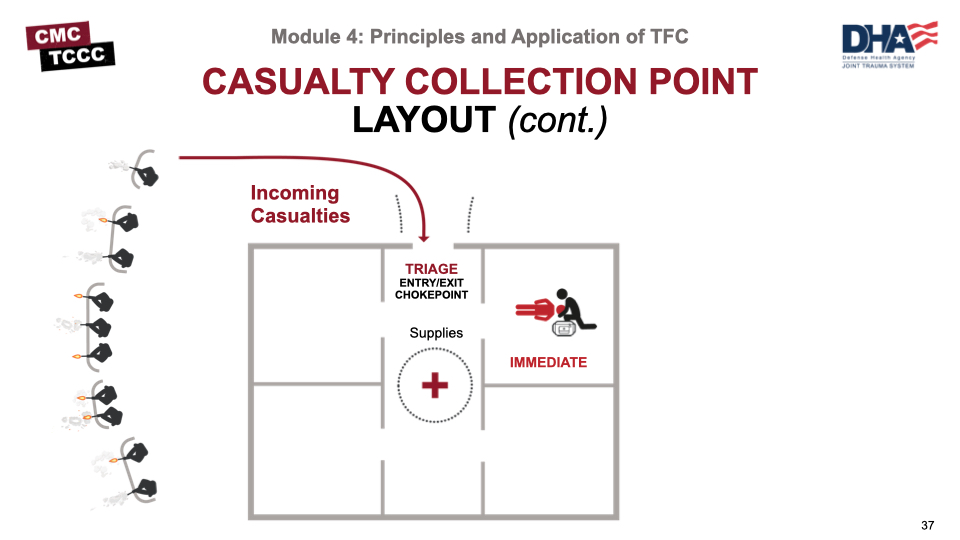
IMMEDIATE
These casualties require an immediate lifesaving intervention (LSI) and/or surgery. Put simply, if medical attention is not provided, they will die. The key to successful triage is to locate these individuals as quickly as possible.
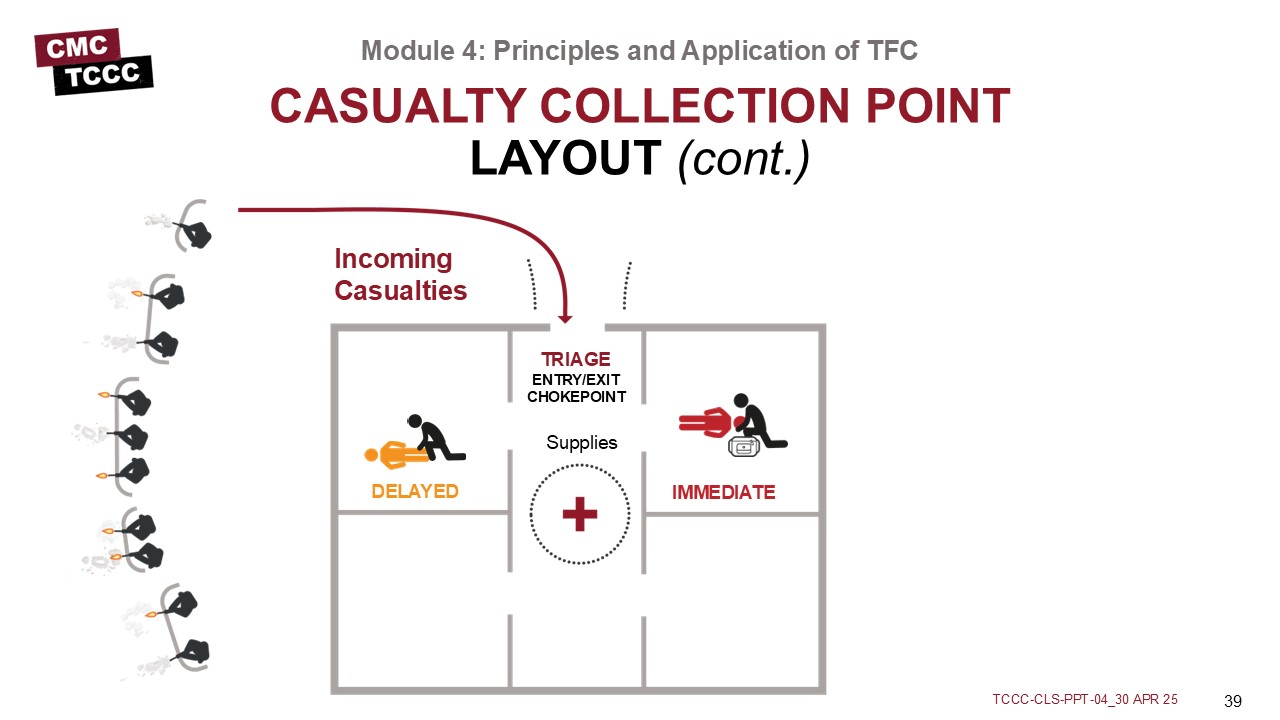
DELAYED
This category includes those wounded who are likely to need surgery but whose general condition permits delay in surgical treatment without unduly endangering the life, limb, or eyesight of the casualty. Sustaining treatment will be required (e.g., oral or IV fluids, splinting, administration of antibiotics, and pain control) but can possibly wait.
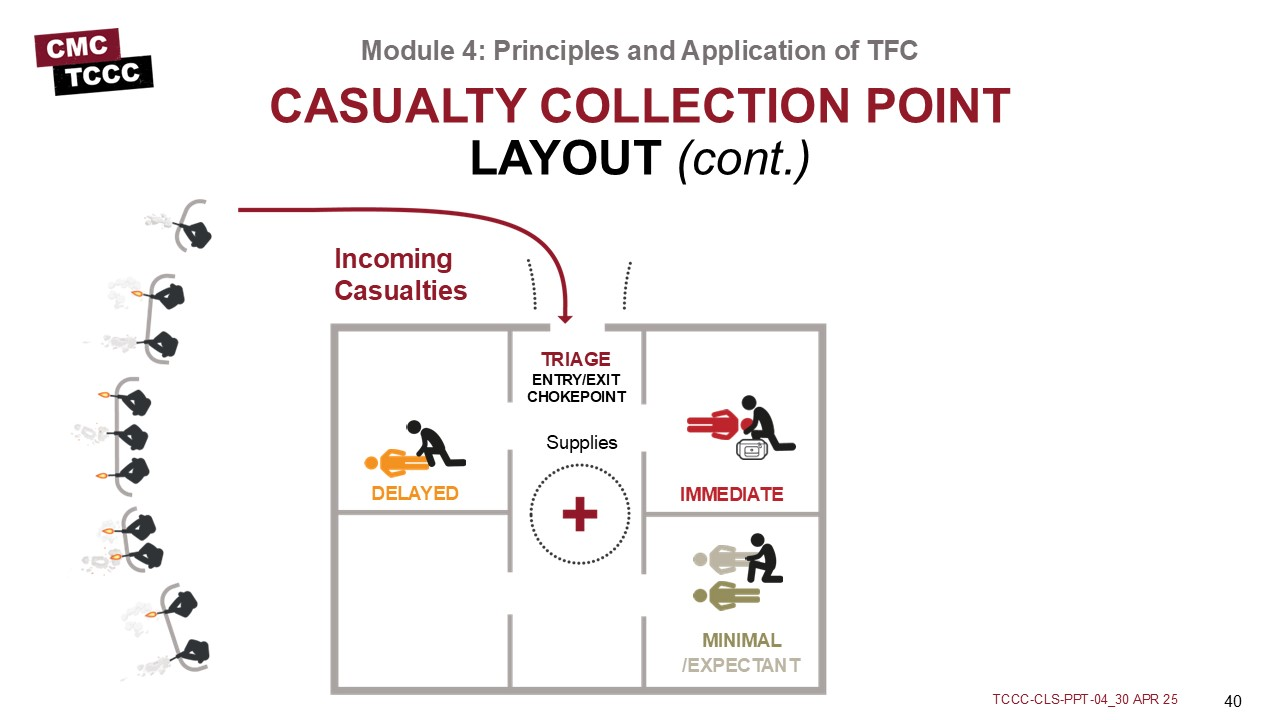
MINIMAL
Casualties in this category are often referred as the “walking wounded.” Although these patients may appear to be in bad shape at first, it is their physiologic state that tells the true story. Casualties who fit into the minimal category may not present themselves until late in the triage process.
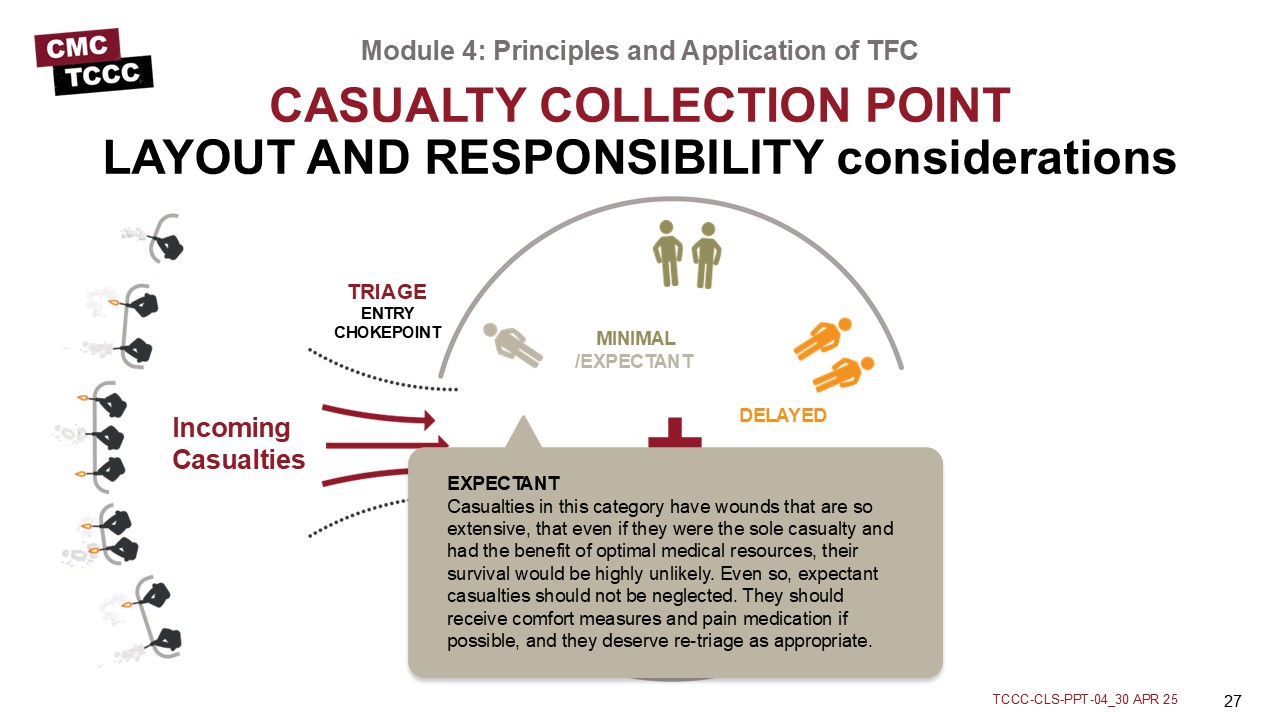
EXPECTANT
Casualties in this category have wounds that are so extensive, that even if they were the sole casualty and had the benefit of optimal medical resources, their survival would be highly unlikely. Even so, expectant casualties should not be neglected. They should receive comfort measures and pain medication if possible, and they deserve retriage as appropriate.
Medical personnel are responsible for everything inside the CCP, including triage, casualty treatment and monitoring, packaging and staging casualties for evacuation, requesting assistance as needed from other unit assets, providing guidance and recommendations to leadership on casualty management and evacuation, medical equipment and supplies.
In an ideal layout, there are separate entry and exit points (which are potential chokepoints) to control casualty flow through the CCP, similar to what is seen in this example.
Unit leadership will determine where the pre-stage evacuation area will be placed as well as secure the MEDEVAC/ TACEVAC zone.
The medic is in charge of categorizing the casualties by evacuation category (Urgent, Priority, Routine).
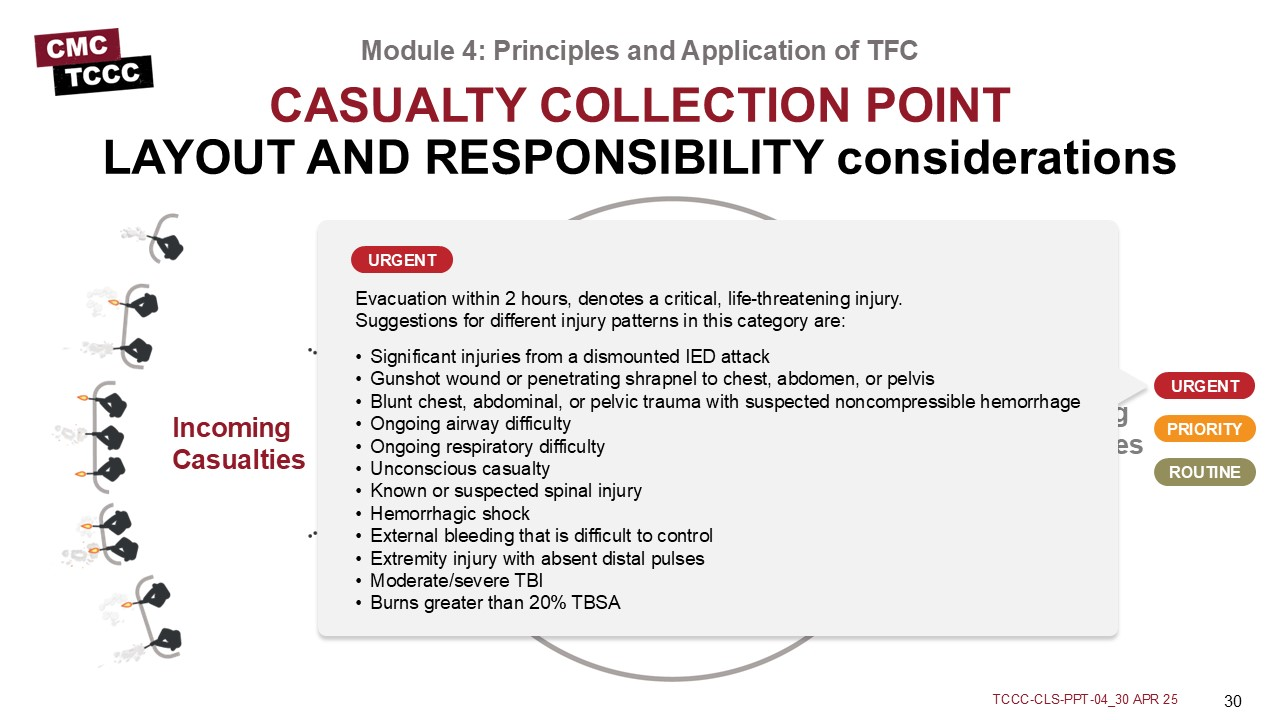
URGENT
Evacuation within 2 hours, denotes a critical, life-threatening injury. Suggestions for different injury patterns in this category are:
- Significant injuries from a dismounted IED attack
- Gunshot wound or penetrating shrapnel to chest, abdomen, or pelvis
- Blunt chest, abdominal, or pelvic trauma with suspected noncompressible hemorrhage
- Ongoing airway difficulty
- Ongoing respiratory difficulty
- Unconscious casualty
- Known or suspected spinal injury
- Hemorrhagic shock
- External bleeding that is difficult to control
- Extremity injury with absent distal pulses
- Moderate/severe TBI
- Burns greater than 20% TBSA
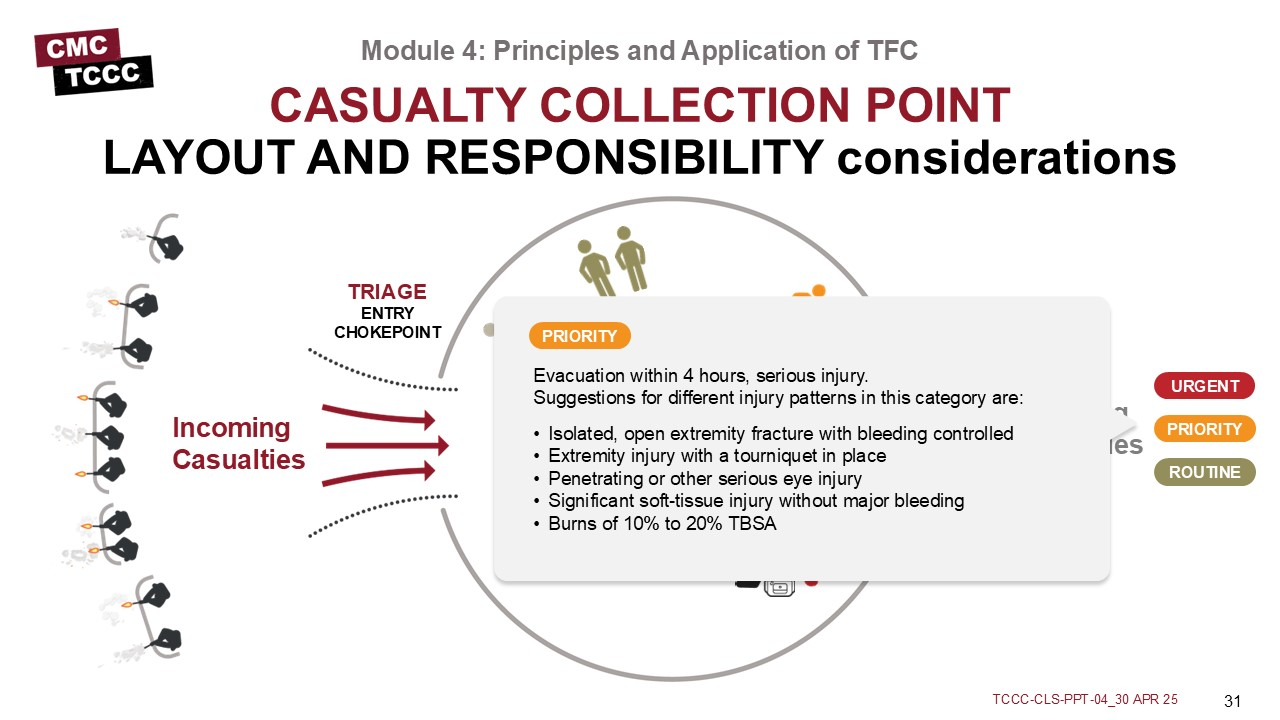
PRIORITY
Evacuation within 4 hours, serious injury. Suggestions for different injury patterns in this category are:
- Isolated, open extremity fracture with bleeding controlled
- Extremity injury with a tourniquet in place
- Penetrating or other serious eye injury
- Significant soft-tissue injury without major bleeding
- Burns of 10% to 20% TBSA
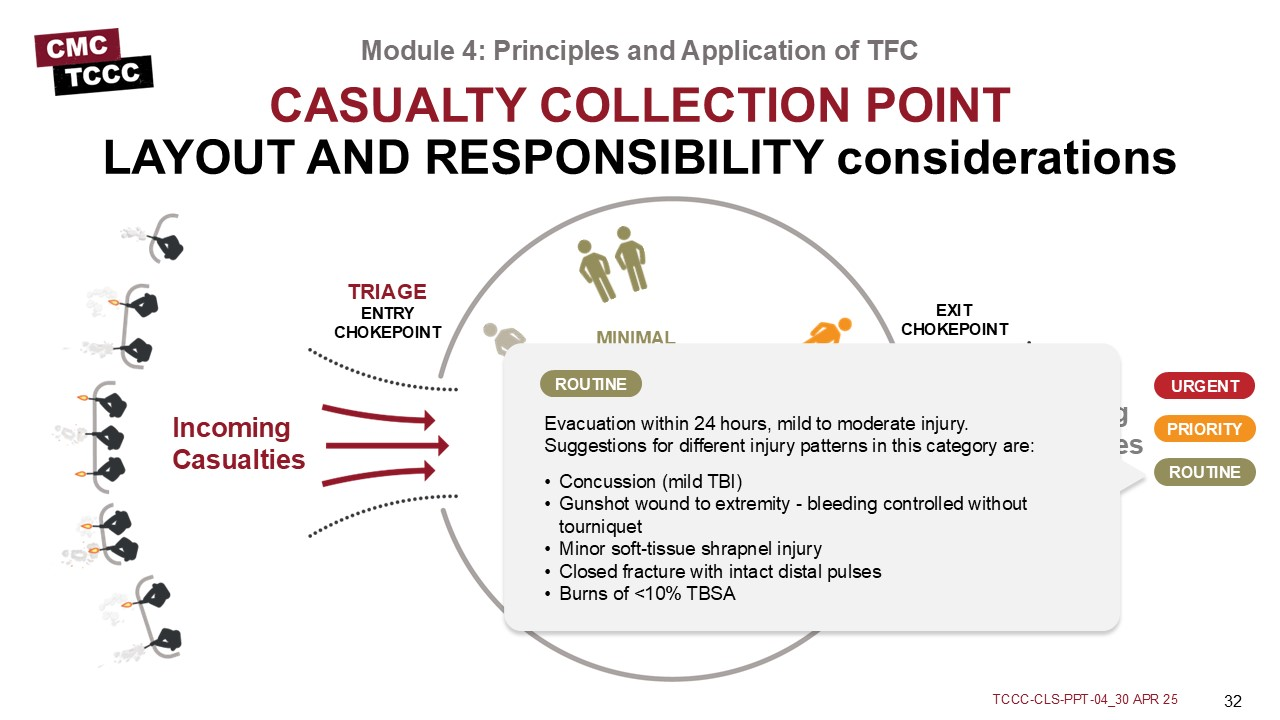
ROUTINE
Evacuation within 24 hours, mild to moderate injury. Suggestions for different injury patterns in this category are:
- Concussion (mild TBI)
- Gunshot wound to extremity - bleeding controlled without tourniquet
- Minor soft-tissue shrapnel injury
- Closed fracture with intact distal pulses
- Burns of <10% TBSA
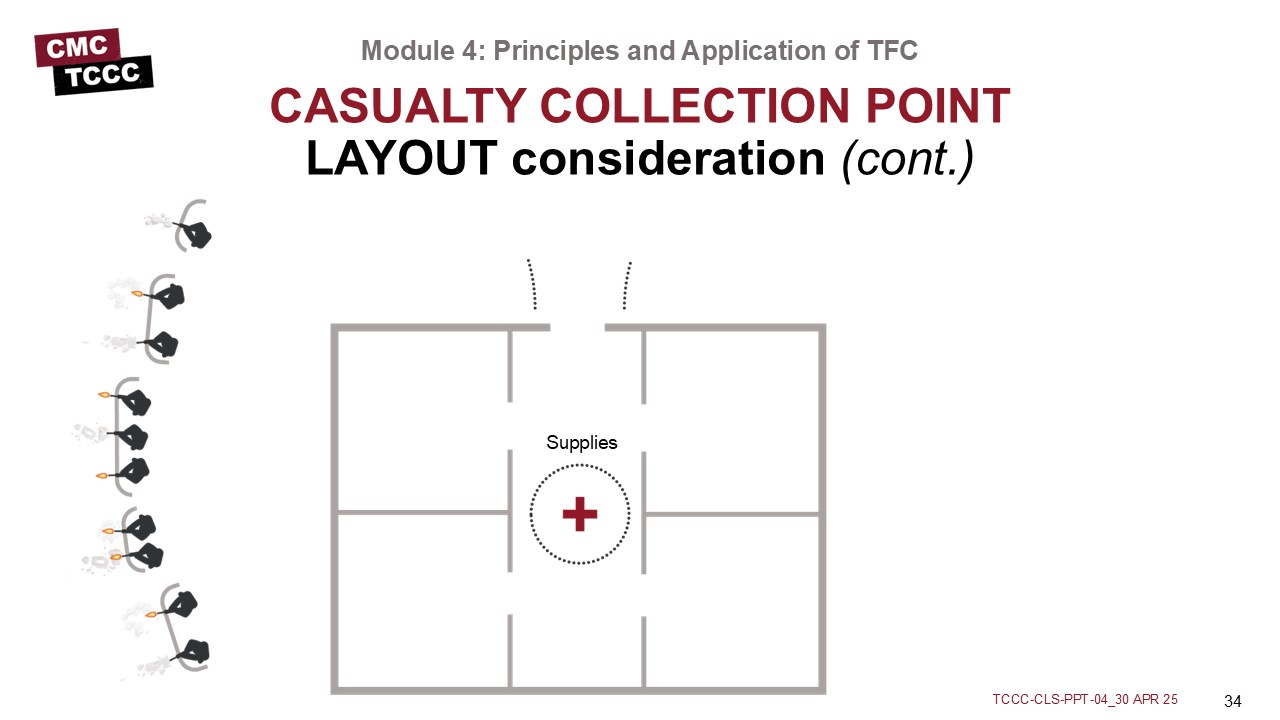
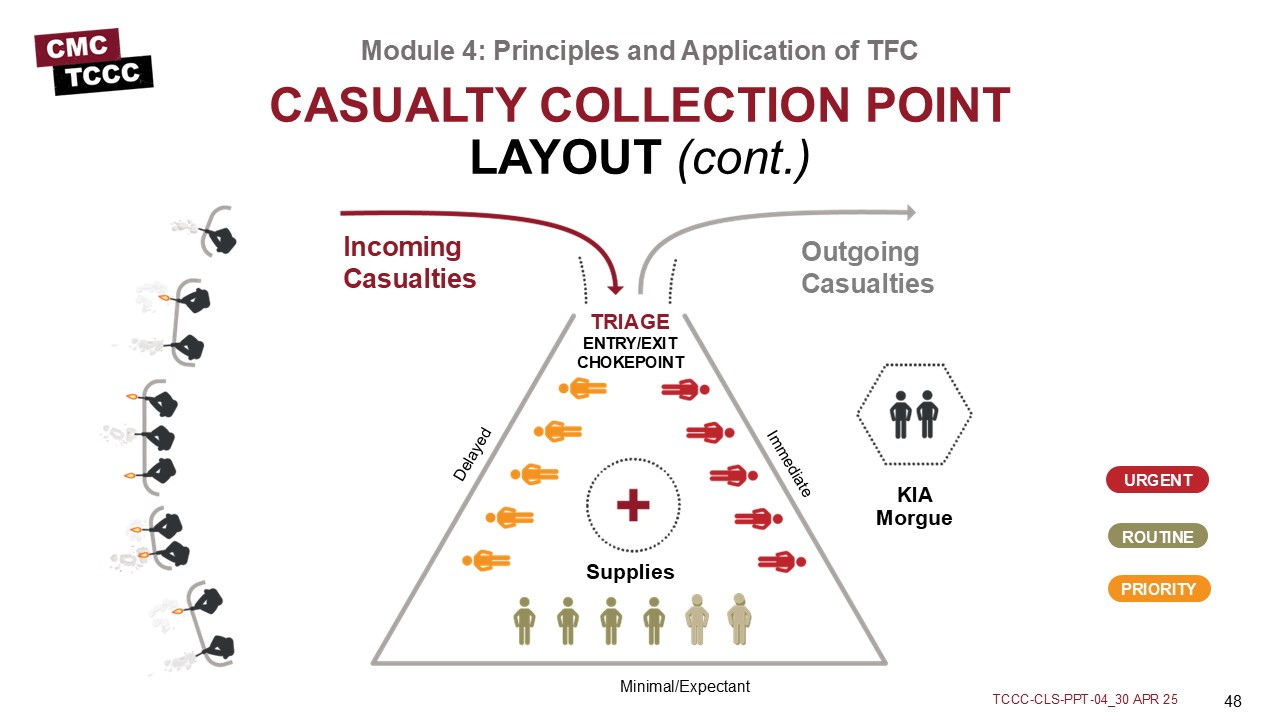
Not every situation allows for separate entry and exit points (as seen in the first example); it is easy to see how having a single entry and exit point for the CCP could create a problem with casualty flow if casualties continue to arrive as others are being moved out to the evacuation point.
Nonmedical unit leadership are typically responsible for security, casualty flow and movement, and everything outside of the CPP. Also, they are responsible for providing assistance to medics with augmentation, directing aid and litter teams, gathering and redistributing casualty equipment and sensitive items, providing accountability and reporting to higher authority, requesting evacuation and establishing CASEVAC or MEDEVAC link-up points, and managing KIA remains.
Medical personnel are responsible for everything inside the CCP, including triage, casualty treatment and monitoring, packaging and staging casualties for evacuation, requesting assistance as needed from other unit assets, providing guidance and recommendations to leadership on casualty management and evacuation, medical equipment and supplies.
In an ideal layout, there are separate entry and exit points (which are potential chokepoints) to control casualty flow through the CCP, similar to what is seen in this example.
Establish a security perimeter in accordance with unit tactical standard operating procedures and/or battle drills.
Casualty movement will be provided by unit personnel in accordance with unit tactical operating procedures and/or battle drills.
Triage/chokepoint will be unit leadership categorizing patients.
IMMEDIATE
These casualties require an immediate lifesaving intervention (LSI) and/or surgery. Put simply, if medical attention is not provided they will die. The key to successful triage is to locate these individuals as quickly as possible.
DELAYED
This category includes those wounded who are likely to need surgery but whose general condition permits delay in surgical treatment without unduly endangering the life, limb, or eyesight of the casualty. Sustaining treatment will be required (e.g., oral or IV fluids, splinting, administration of antibiotics and pain control) but can possibly wait.
MINIMAL
Casualties in this category are often referred as the “walking wounded.” Although these patients may appear to be in bad shape at first, it is their physiologic state that tells the true story. Casualties who fit into the minimal category may not present themselves until late in the triage process.
EXPECTANT
Casualties in this category have wounds that are so extensive, that even if they were the sole casualty and had the benefit of optimal medical resources, their survival would be highly unlikely. Even so, expectant casualties should not be neglected. They should receive comfort measures and pain medication if possible, and they deserve re-triage as appropriate.
KIA Morgue should be out of sight from casualties suffering life-threatening trauma. Ensure to have at least one first responder present to protect and guard KIA personnel.
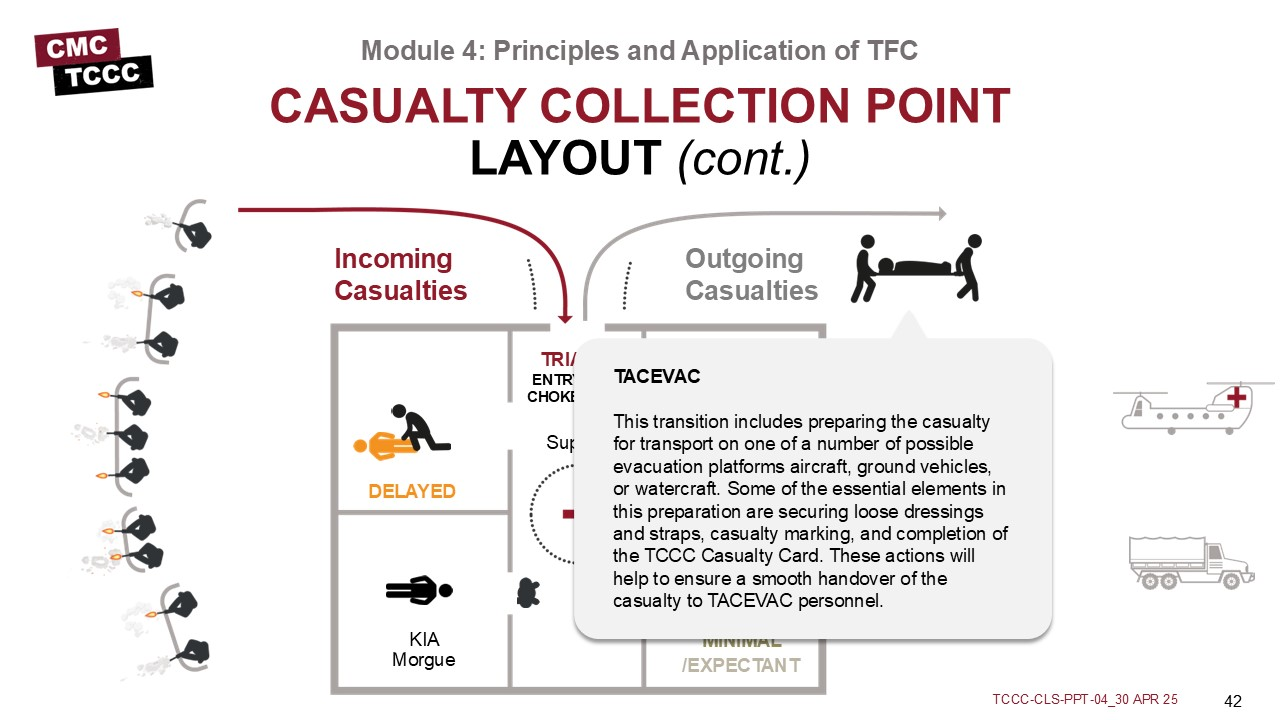
This transition includes preparing the casualty for transport on one of a number of possible evacuation platforms aircraft, ground vehicles, or water craft. Some of the essential elements in this preparation are securing loose dressings and straps, casualty marking, and completion of the TCCC Casualty Card. These actions will help to ensure a smooth handover of the casualty to TACEVAC personnel.
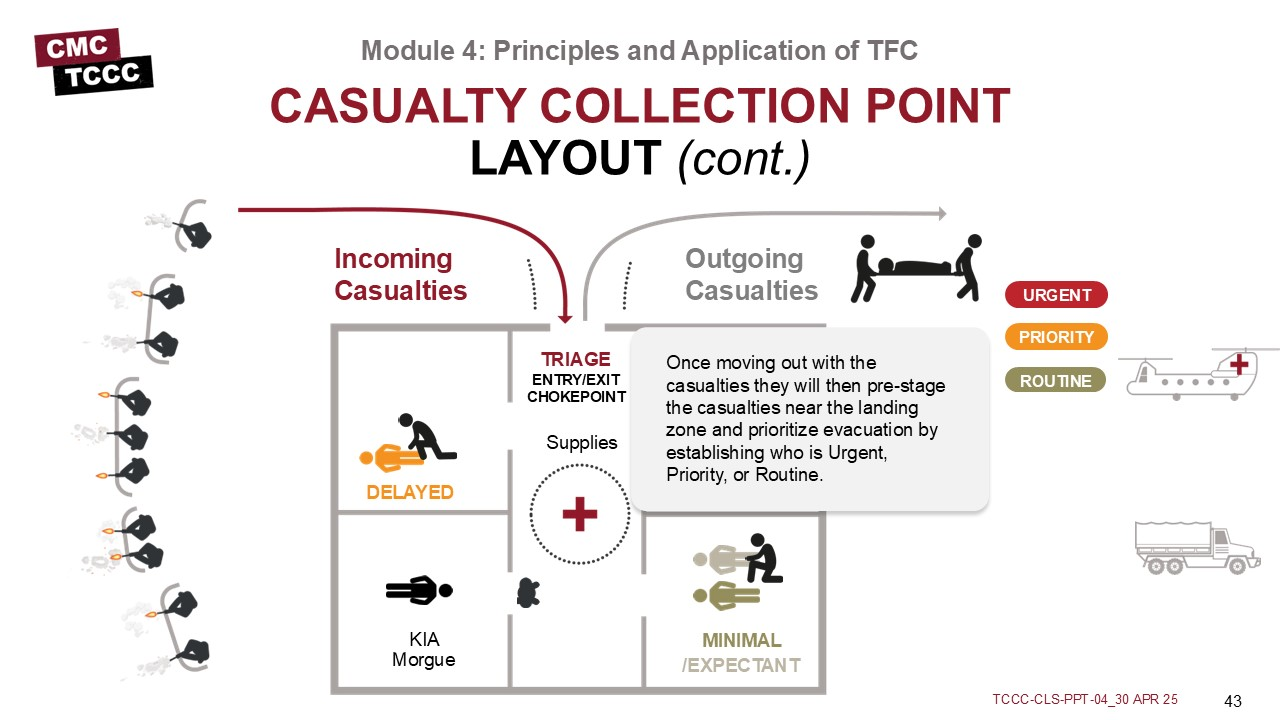
Once moving out with the casualties they will then pre-stage the casualties near the landing zone and prioritize evacuation by establishing who is Urgent, Priority, or Routine.
Medically regulated casualty movement using dedicated medical evacuation platforms. These are crewed by medical attendants and generally have more medical treatment equipment available than nonmedical platforms. MEDEVAC platforms are predesignated assets that bear Red Cross markings and carry no offensive weaponry such as rockets or missiles. MEDEVAC movements may include both clearing casualties from the battlefield and moving casualties between medical treatment facilities.
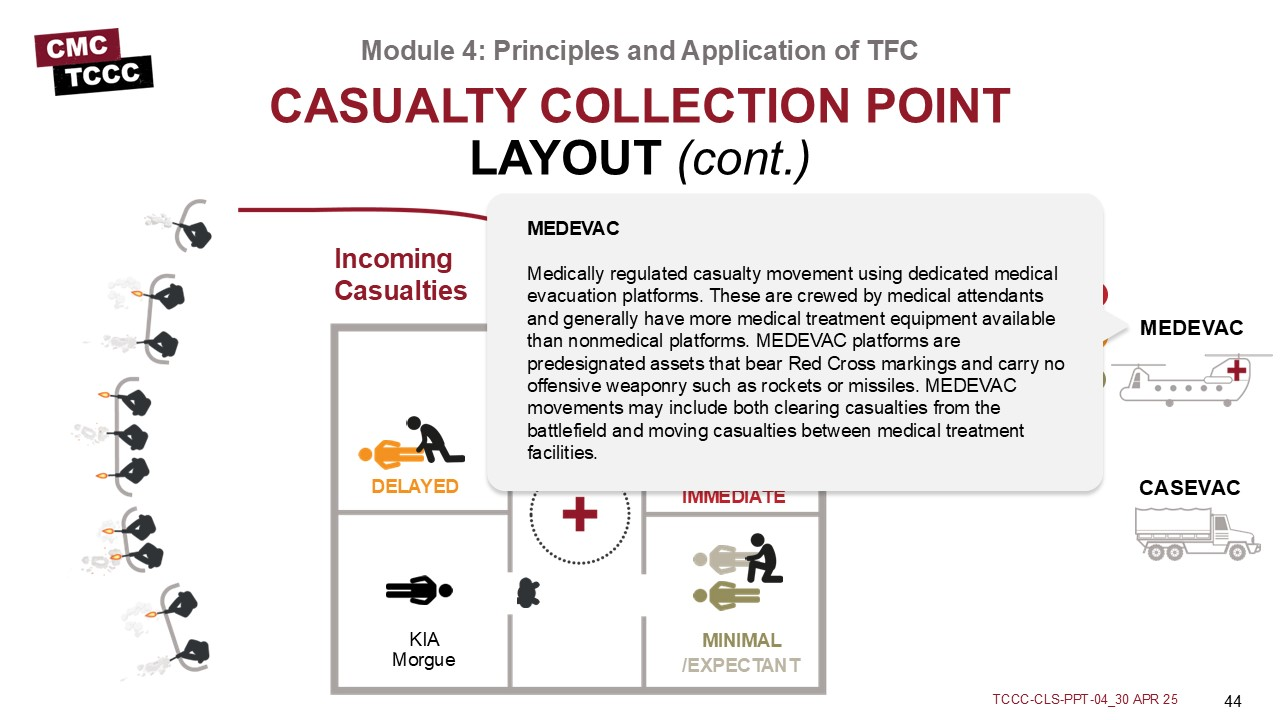
The unregulated movement of casualties from the point of wounding to the first point of surgical care (Role 2 Forward Surgical Team or Role 3 Combat Support Hospital). CASEVAC platforms are typically armed tactical assets that bear no Red Cross markings. These may be aircraft, vehicles, or maritime vessels of opportunity.
Medical personnel are responsible for everything inside the CCP, including triage, casualty treatment and monitoring, packaging and staging casualties for evacuation, requesting assistance as needed from other unit assets, providing guidance and recommendations to leadership on casualty management and evacuation, medical equipment and supplies.
In an ideal layout, there are separate entry and exit points (which are potential chokepoints) to control casualty flow through the CCP, similar to what is seen in this example.
There are several different examples of potential CCP layouts since each situation is different and the exact configuration will vary based upon unit SOPs, mission, tactical situation, terrain, etc.; but the layout of a CCP follows certain principles.
Tactical Field Care is the care rendered once the combat medic/corpsman and casualty are no longer under direct threat from effective enemy fire. This allows for the time and the relative safety for a more deliberate approach to casualty assessment and treatment.
The tactical situation is fluid and can change quickly. Maintain situational awareness. Establish a security perimeter in accordance with unit standard operating procedures and/or battle drills. Casualties with altered mental status should be disarmed and weapons communications equipment, and other sensitive items should be secured/redistributed.
In the Tactical Field Care phase, MARCH PAWS is followed for a more deliberate approach to the assessment and treatment of casualties than was possible during Care Under Fire. A full tactical trauma assessment should follow the steps of the MARCH PAWS sequence.
In TFC the Combat Medic/Corpsman should communicate with the casualty throughout assessment and treatment, communicate with other first responders, Combat Lifesavers, and medical providers regarding casualty assessment and treatment (using the DD 1380), communicate casualty status and evacuation requirements with tactical leadership, and communicate with the evacuation system (TACEVAC) including 9-line MEDEVAC requests and MIST reports.
When there are multiple casualties, the combat medic/corpsman may need to triage casualties into prioritized treatment groups (immediate, delayed, minimal, expectant) based upon severity of injuries prior to providing or assisting other first responders, combat lifesavers, and medical personnel with casualty care. The Combat Medic/Corpsman should consider MARCH in deciding how to prioritize treatment and evacuation of multiple casualties in the TFC phase of care.
The Casualty Collection Points (CCPs) should be established reasonably close to the fight where casualties are likely to occur, be near natural “lines of drift”, provide relative cover and concealment from the enemy whenever possible, and have access to evacuation routes.
To close out this module, check your learning with the questions below (answers under the image).
Answers
What is the difference between TFC and CUF?
Tactical Field Care is the care rendered once the combat medic/corpsman and casualty are no longer under direct threat from effective enemy fire. This allows for the time and the relative safety for a more deliberate approach to casualty assessment and treatment.
True or False: During TFC, the tactical situation could change back to CUF again at any time?
True
What is MARCH PAWS?
In the Tactical Field Care phase, the MARCH PAWS sequence is followed for a more deliberate approach to the assessment and treatment of casualties than was possible during Care Under Fire. A full tactical trauma assessment should follow the steps of the MARCH PAWS sequence.
What is triage?
Triage is the deliberate sorting of casualties and allocation of limited treatment resources according to a system of priorities designed to maximize the number of survivors on the battlefield.
What is a CCP?
The Casualty Collection Point (CCP) is a location on the battlefield for the triage, treatment and monitoring, and the packaging/staging of casualties for evacuation. The CCP should be established reasonably close to the fight where casualties are likely to occur, be near natural “lines of drift”, provide relative cover and concealment from the enemy whenever possible, and have access to evacuation routes.
Throughout the course, you’ll note several references, but keep in mind that the TCCC Guidelines are the core guidance for assessing and treating casualties in a TCCC setting, as well as the emphasis for training. Likewise, the Prehospital Trauma Life Support (PHTLS)., Military Edition, teaches and reinforces the principles of rapidly assessing a trauma patient using an orderly approach.