Orthopaedic Trauma: Extremity Fractures
Joint Trauma System
Orthopaedic Trauma: Extremity Fractures
GOALS
The purpose of this CPG is to describe the initial non-surgical and surgical management of extremity fractures; to demonstrate appropriate application of an external fixator with limited resources in order to stabilize for transport; and to define care guidelines for fractures of upper and lower extremities in the context of the host nation’s environment and the options available to different patient groups.
BACKGROUND
The majority of combat casualties sustain musculoskeletal injuries1,2 and the treatment of fractures and associated soft tissue wounds comprise the majority of Role 2 and 3 orthopaedic procedures.3 The prevalence of musculoskeletal injury requires that surgeons caring for victims of war must manage extremity fractures in the austere environment. Prior to the development of long bone stabilization, mortality from isolated femur fractures was 87% in WWI and reduced to <8% with appropriate splinting. During the recent conflicts, especially as surgical teams have gotten smaller and more dispersed, long bone extremity fracture stabilization will occasionally take second precedent to other injuries. The cumulative burden of femur fractures can make polytrauma patients sicker; so while resources such as imaging may be limited, early femur stabilization is critical for the overall outcomes. Appropriate wound management and fracture stabilization are the mainstays of treatment and are a critical aspect of the multidisciplinary treatment of combat casualties. While a patient’s overall physiology and associated wounds must be considered, the effective stabilization of long bone fractures and appropriate debridement of soft tissue injury contribute to effective resuscitation.
Evaluation and Treatment
Early and Thorough Wound Debridement
- Prehospital care of extremity wounds is covered in the Tactical Combat Casualty Care guidelines and in the Acute Traumatic Wound Management in Prolonged Field Care CPG, 24 Jul 2017. In general, suspected fractures should be splinted whenever possible once life-threatening injuries have been addressed. Open wounds should be treated as soon as possible with antibiotics; either oral or IV antibiotics are acceptable depending on the situation and the patient’s ability to swallow the medication. Traction splints may be utilized for femur fractures, however, are not required and other splinting methods may be more expedient. A pelvic binder is indicated in cases of severe lower extremity injury and may be utilized in conjunction with a traction splint.
- Far-forward medical facilities may not have the capability to perform surgical debridement, but early irrigation with removal of gross contaminants may be possible at any level of care and should be performed as soon as possible after injury.
- During the initial examination, the neurologic and vascular exam of the affected extremities should be carefully documented and the affected extremity evaluated for signs of acute compartment syndrome (ACS). Accurate documentation for the next role of care is necessary to determine any evolution of ACS or neurovascular injury.
- A thorough irrigation and surgical debridement should be performed as early as possible.4
- Remove debris and devitalized tissue.
- Bone fragments without soft tissue attachment (i.e. muscle, periosteum) or that are easily removed, should be excised with the exception of large articular fragments.
- All viable tissue should be preserved in order to afford receiving physicians the greatest number of reconstructive options.
- Tag transected nerves and tendons to facilitate identification of structures during reconstruction.
- Treat open fractures with prophylactic antibiotics, primarily 1st generation cephalosporin and tetanus toxoid as soon as possible.5-9 While there currently is no evidence to support broader spectrum antibiotics, Gram negative organisms are commonly cultured initially and during the treatment of subsequent infection.10 The use of topical antibiotics is becoming more prevalent and has been shown effective in preventing subsequent infection.11
Fracture Stabilization
- Fracture instability, especially long bone, can compromise effective patient resuscitation due to ongoing hemorrhage, continued soft tissue damage and respiratory splinting from increased pain. This leads to increased cytokine release, inflammatory response, and shock.12-15 Early stabilization of femoral shaft fractures is associated with decreased pulmonary complications (including acute respiratory distress syndrome), ICU time, hospital days and mortality and others.16-19 Long bone stabilization is an important part of early damage control surgery by stabilizing both anatomy and physiology, and is required in the setting of a temporary shunting or definitive vascular repair. Splinting may be the only far-forward option for fracture stabilization and affords the receiving surgeon the greatest number of surgical options. Splinting also may be the most appropriate intervention for low energy fractures and those in the upper extremity and distal lower extremity such as wrist, hand, humerus, elbow, ankle, and foot fractures. An appropriate splint can be effective in temporizing any suspected or known fracture or soft tissue injury until more appropriate stabilization or imaging is available.
- Open wounds should be addressed first and the status of the underlying wound as well as the date and time of the most recent debridement and irrigation should be documented on the splint itself. If the patient is to be transported, splints must be suitable for the mode of transportation and acceptable within limits of passenger space. Caution should be utilized so splints are not constrictive/circumferential or predispose to compartment syndrome, especially prior to long evacuations. Splints should immobilize the joint above and below the fracture and should have adequate padding at pressure points to prevent soft tissue injury. Splints are intended to limit further injury and are not meant to be definitive treatment. Anatomic reduction may not be possible or necessary for initial splinting of fractures, but a restoration of overall length and alignment of the limb should be sought. A neurovascular exam, including assessing for compartment syndrome, should be documented pre- and post-splinting with or without reduction attempts, to confirm that perfusion and function remain intact after fracture manipulation.
- Finger and hand injuries may be immobilized with standard splinting methods. Forearm and elbow injuries are best splinted with a long arm posterior splint or a sugar-tong splint. Humerus and shoulder fractures are best immobilized using a sling and swathe or coaptation splint, ensuring there is enough padding at the axilla. Long leg splints for tibia fractures and below the knee splints for ankle and foot fractures provide adequate stability for transport. Ensure the splint padding allows access for limb compartment.
External Fixation
1. Due to logistical constraints and concern for infection, internal fixation is not recommended in most austere settings where evacuation to higher levels of care is possible. Surgeons should be well versed on external fixator placement for long bone and periarticular fractures.
In the setting of concomitant vascular injuries requiring repair or shunting, the orthopaedic surgeon and general surgeon should discuss the sequence of external fixation application (before or after the vascular procedure) considering the following:
- Ischemia time
- Degree of deformity in the fractured extremity, specifically the amount of shortening, angulation, mal-rotation, and instability across the fracture site
- Surgeon comfort level and experience affecting speed of external fixation application
- Indications to proceed directly to arterial repair versus need for initial shunting
Benefits of early vascular shunting or repair include reduced ischemia time and possibly reduced need for distal limb fasciotomies, while early fracture stabilization helps re-establish limb and vascular length across the site of injury as well as restore tissue planes for dissection and exposure. The treating surgeons should be mindful of the effects of restoring limb length and alignment on the vascular shunt/repair and plan their interventions to avoid disruption of restored blood flow while effectively stabilizing the limb.
2. External fixation affords adequate fracture stabilization to minimize additional soft tissue trauma and can provide easier access for wound care and re-evaluation for neurovascular injury and ACS. Early fracture stabilization may blunt inflammatory mediators associated with fractures in poly-trauma12,18 and can be rapidly applied in the multiple injured patient or in a mass casualty situation. Stability afforded by external fixation is also beneficial for pain control and ease of transport, and minimizes the need to manipulate the injured limb during transport and at each higher role of care.
3. External fixation in the austere environment is performed within the constraints of limited equipment and the lack of available fluoroscopy. Surgeons should be familiar with extremity bone and neurovascular anatomy in order to safely apply an external fixator for initial stabilization without the aid of fluoroscopy. Otherwise, splinting should be used for temporary stabilization. Specific portable external fixation kits designed for military use include self-drilling and self-tapping pins that use hand-powered drills for advancement into the bone. External fixation has been shown to be safe in the austere environment when performed at Role 2 and Role 3 facilities.20 However, caution is advised in attempting external fixation when no basic radiographic imaging is available to identify the fracture pattern, particularly for closed fractures where the facture pattern cannot be visualized or palpated through an open wound. In this case the limb should be splinted without traction and the patient moved to a level of care that has X-Ray capability.
4. External fixator stability is improved by increasing bony apposition at the fracture site, placing the connecting bars as close to the skin as is deemed safe, increasing the distance between pins in each fracture fragment, and using the largest diameter pin possible (typically, 5.0 mm pins in long bones). Two appropriately placed pins; above and below fracture fragment should provide sufficient stability and will allow receiving surgeons the most options for definitive fixation. Consider the skin incisions for future internal fixation plans when choosing pin sites.
5. The following guidelines allow the safe and effective placement of fixation pins in the austere environment, without the assistance of fluoroscopy but with some basic imaging of the fracture pattern available prior to pin placement.21 Pins should be placed both “near and far” from the fracture in both major bone fragments. The fracture ends in a closed fracture can be estimated by palpation/manipulation of the bone. One pin in each main fracture fragment should be placed typically 2-3 cm away from the fracture end to improve stability. Pins placed too near the fracture can decrease the external fixator’s ability to maintain stability if the pin only captures one bone cortex or is placed in fracture lines that are not grossly apparent. To place each pin, make a longitudinal incision approximately 1 cm in length at the planned pin site and bluntly dissect down to bone. The incision should be generous enough to accommodate the entire width of the pin, as trapped or tented skin contributes to skin irritation and pin tract infection, ultimately leading to pin loosening. Load the pin in either a powered drill or manual driver and place the pin into the incision until the pin meets bone. The pin tip can be used to palpate the edges or curve of the bone so that the central portion may be identified. After broaching the near cortex, hand advancement of the pin should be used to allow the surgeon to feel the far cortex, which is identified by encountering increased resistance while turning the pin. Engaging pin threads across the far cortex provides ideal stability. If intraoperative imaging is available, pins should be advanced until the drill tip is fully past the far cortex. If fluoroscopy is not available, manual advancement 6-8 full turns after reaching the inner surface the far cortex should provide sufficient engagement of the pin. Surgeons must always be aware of limb anatomy as excessive pin advancement can put neurovascular structures at risk.
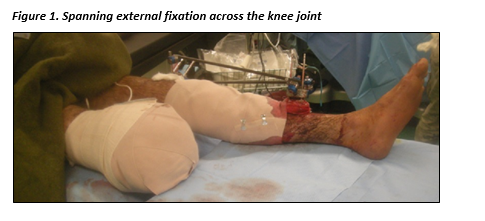
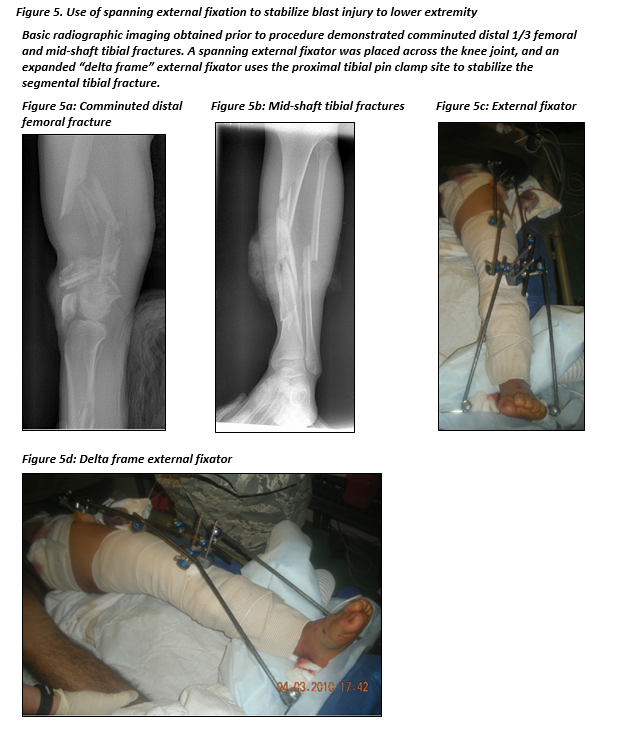
6. The “far” pins should be placed as far from the fracture site as deemed safe. Intercalary fragments of segmental long bone fractures typically do not require pin fixation, and single pin fixation in these smaller fragments likely does not add to construct stability. Clamps designed to connect the pins and bars are available in the equipment sets, and the pin clamp may be used as a drill guide for appropriate placement of incisions between pin sites. However, using these clamps limits the potential distance between pins in a fracture segment and off-axis pins may not engage in the clamp sufficiently to the detriment of construct stability. External fixators may be placed to span joints if the fractures is near a joint or extends into the articular surface (knee, elbow). (Figures 1, 5, 6)
7. After placing pins, the pins in each fragment can be secured to each other with a pin clamp and tightened. Modified bars are then secured into each pin clamp, and long bars connect to the modified bars of each pin clamp/fracture fragment by using “bar-to-bar” connectors. One bar spanning each fracture fragment is often sufficient for fracture stability. If bar length is too short to span the fracture site, then 2 bars can be connected by a “bar-to-bar” clamp to gain the necessary length. The overall goal of any construct is to restore length and overall alignment of the limb by establishing a provisional reduction of the fracture (thus improving stability), reduce intracompartmental volume to allow tamponade of bleeding, and to restore vascular flow by “unkinking” vessels. Without fluoroscopy, simple longitudinal traction while grossly restoring coronal and sagittal alignment is sufficient for initial stabilization. When spanning the knee, the fixator should be tightened with slight knee flexion. (See Figure 1 below.)
8. Pins can be dressed with Xeroform or similar material and gauze, with Kerlex wrapping of the pins to provide stability to the skin. No formal pin care is recommended, especially in this acute phase, as formal cleaning protocols have failed to demonstrate improvement in pain, stability, or complications.22
Lower Extremity
Femur: Given the medial and posterior location of neurovascular structures in the thigh, an anterolateral or lateral approach can be used with little risk to neurovascular structures. At the distal third of the femur, however, care should to be taken to avoid over-penetration of the posterior cortex, as this risks injury to the popliteal artery. Anterior pins placed in the distal femur should begin 7.5 cm above the superior pole of the patella to avoid inadvertent intraarticular placement.23
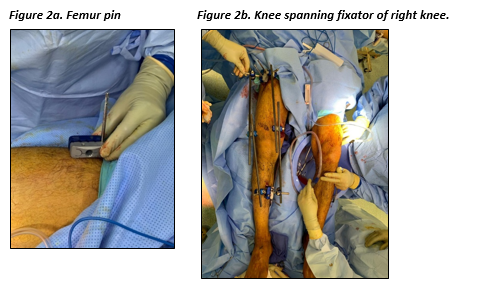
Knee: For distal femur and/or proximal tibia fractures including those involving the articular surfaces, a knee spanning fixator is most appropriate. Two pins each in the intact femur and tibia can be connected by bars. To maximize stability of this longer construct, good pin spread and/or multiple bars should be considered. As with other long bone fractures, longitudinal traction is used to correct coronal and sagittal alignment. The fixator should be locked with the knee in flexion. A posterior slab, short leg splint can be helpful to control ankle plantarflexion and provide additional soft tissue rest and pain control as the gastrocnemius muscle crosses the knee joint.
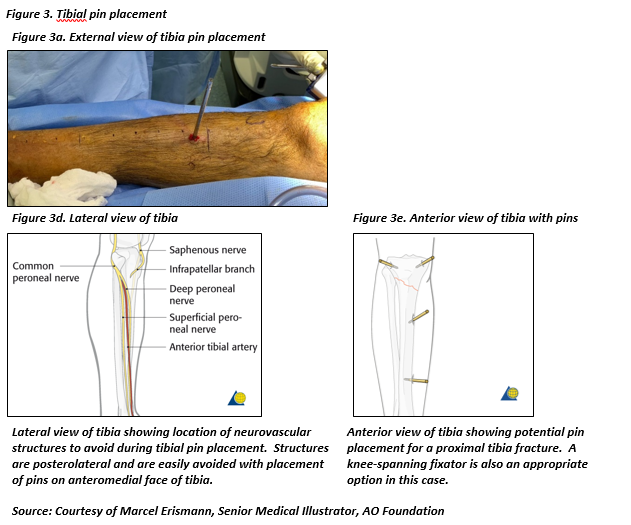
Tibia: The neurovascular bundle runs along the bone’s posterolateral surface. This leaves the anteromedial surface free for safe pin placement. The thin layer of subcutaneous tissue overlying the bone makes this surface easily palpable along its entire length. The direct anterior tibial crest should be avoided as it is significantly thicker than the rest of the bone, and pin placement is difficult even with a power drill. Pins should be placed about 1 cm medial to the anterior crest to avoid the crest as excessive drilling can result in thermal necrosis, pin loosening and eventual infection.
Fibula: External fixation of the fibula is not indicated despite any amount of associated tibia or soft tissue injury.
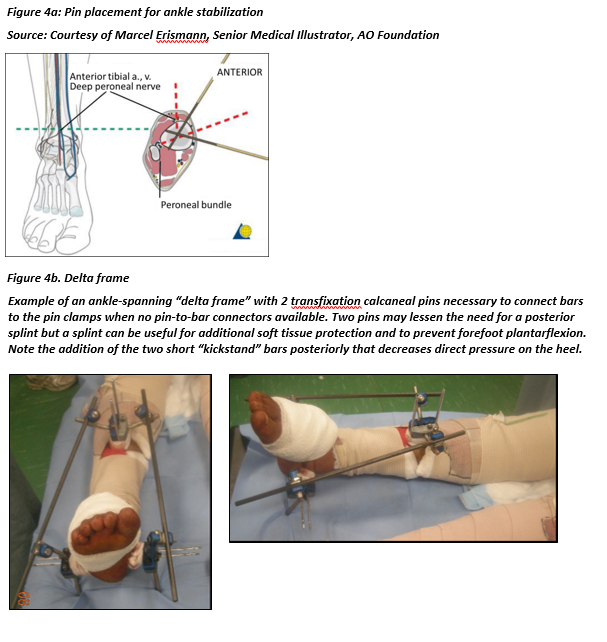
Ankle: To stabilize the ankle (typically in the setting of an unstable distal tibia fracture), two pins should be placed in the tibia proximal to the fracture site and be connected to a centrally-threaded transfixation pin (or pins) placed through the calcaneus using a medial-to-lateral approach to avoid injury to the neurovascular bundle located just posterior to the medial malleolus. (Figure 4a below) While a 4 mm pin can be placed in the first metatarsal to control ankle dorsiflexion, stable placement can be difficult and the tibialis anterior tendon at the base of the bone can be at risk. A calcaneal pin is more easily placed, and sufficient ankle dorsiflexion can be maintained with the addition of a posterior slab splint as necessary. Talar neck pins, with appropriate anatomic knowledge, can be useful to stabilize the distal tibia, particularly if a calcaneal fracture is present that precludes transfixation pin placement.
Upper Extremity
Splinting of the upper extremity may be preferable over external fixation especially for isolated injuries. Upper extremity external fixators can be complicated by the proximity of neurovascular structures. Familiarity with upper extremity anatomy and careful dissection before pin placement can lessen the chance of injury.
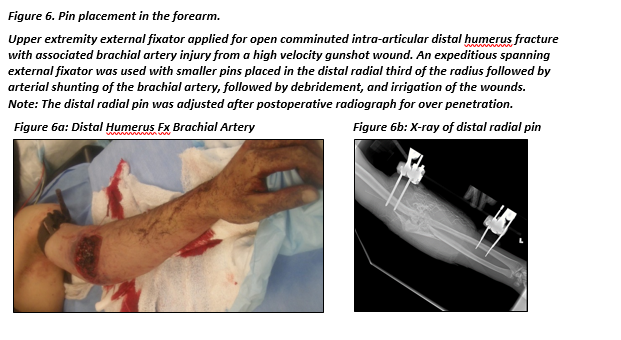
Humerus: External fixation of the humerus can be particularly risky due to the intimate relationship with the neurovascular structures. External fixation should be reserved for instances of severe soft-tissue destruction or when associated vascular injury requires shunting or repair. In general, the lateral and anterior surfaces are safer for half pin insertion. Over-penetration of the medial cortex places the neurovascular bundle at risk for injury. For fixation around the elbow, half pins are placed proximal to the lateral epicondyle through an open approach. The incision should be of sufficient length to positively identify the radial nerve as it traverses anteriorly between the biceps and brachioradialis about 10-14 cm proximal to the lateral epicondyle. After pin placement, the incision is closed around the pins.
Ulna: The dorsal surface of the ulna is easily palpable along its entire length. The ulnar nerve is located radial and volar to the bone making the palpable surface an ideal site for pin placement. 5mm pin diameters can be too large based on the diameter of the bone, and 3-4mm pins should be used instead.
Radius: At the proximal third of the radius, the dorsal surface is obscured by the variable course of the posterior interosseous nerve. Accordingly, pin placement should be limited to the radial surface of the more palpable middle and distal third of the radius to avoid injuring the radial nerve motor branches. An incision allowing sufficient dissection to expose and retract the branches of the superficial branch of the radial nerve and underlying tendons is necessary to avoid entrapment or damage of these structures. As with the ulna, 3-4mm diameter pins are often more appropriate due to the size of the radius at the location the pins are being placed.
Host Nation Casualties
One particular challenge for medical providers in an under-resourced host nation is the likelihood of treating individuals with unknown follow-up care. Low-energy, closed fractures may be treated definitively with a splint or cast. Plaster often is preferred to fiberglass for casting, as cast saws may not be locally available. Certain low-energy fractures may warrant open reduction and internal fixation or closed reduction and percutaneous pinning. External fixation is also an option for initial stabilization if transfer to a host nation facility is possible, or tempo of casualties allows for delayed internal stabilization. External fixation can be used successfully to definitively treat fractures but requires careful pin placement, long term construct stability and close follow up that may not be possible. In the setting of high-energy wounds with extensive soft tissue loss, a staged amputation that may be definitively closed in a short period of time must be considered. Unavailability of prolonged and advanced surgical care make limb salvage challenging.
Performance Improvement (PI) Monitoring
POPULATION OF INTEREST
Patients with long-bone fractures of the extremities (femur, tibia, humerus, radius, ulna).
INTENT (EXPECTED OUTCOMES)
- All patients in the population of interest have a neurovascular exam documented at every role of care.
- All patients in the population of interest have fractures stabilized (splinted or external fixator placement) prior to transport from the first surgical capability.
PERFORMANCE/ADHERENCE METRICS
- All long-bone extremity fractures are stabilized by splinting or external fixation prior to movement from a surgical capability.
- Neurovascular examination is documented for all extremity fractures.
- Casualties with fractures and vascular injury in the same extremity (i.e. vascular injury associated with fracture) who underwent vascular shunt or vascular repair also received external fixation.
- Number and percentage of patients in the population of interest who have a neurovascular exam documented at every role of care.
- Number and percentage of patients in the population of interest who have fractures stabilized (splinted or ex-fixed) prior to transport from first surgical capability.
DATA SOURCE
- Patient Record
- Department of Defense Trauma Registry (DoDTR)
SYSTEM REPORTING & FREQUENCY
The above constitutes the minimum criteria for PI monitoring of this CPG. System reporting will be performed every five years; additional PI monitoring and system reporting maybe performed as needed.
The system review and data analysis will be performed by the JTS Chief and the PI Branch.
RESPONSIBILITIES
It is the trauma team leader’s responsibility to ensure familiarity, appropriate compliance and PI monitoring at the local level with this CPG.
ACKNOWLEDGEMENTS
The JTS extends a special thanks to the voting members of the JTS Committee on Surgical Combat Casualty Care for their contribution to the development and publication of this clinical practice guideline.
JTS Defense Committee on Surgical Combat Casualty Care (CoSCCC)
JTS Chief: COL Stacy A. Shackelford, MD, FACS, USAF, MC
JTS Senior Enlisted Advisor: MSG Michael A. Remley, ATP, SFC, MC, USA
DCoT Chair, CoSCCC Chair: COL Jennifer M. Gurney, MD, FACS, MC, USA
Voting Members, Peer Reviewers
COL Scott B. Armen, MD, FACS, FCCP, FCCM, MC, USAR
COL David Aaron Baker, MD, MC, FS
COL Jay Baker, MD, MC, USA
COL Tyson Becker, MD, MC, USA
CDR Randy S. Bell MD, FAANS, MC, USN
PO1 Jeffrey D. Bentley, USN USA
Lt Col Craig (CJ ) Berg, MD, USAF, MC
CDR Virginia Schmied Blackman, PhD, RN, USN
CAPT Matthew Bradley, MD, MC, USN
Col Jeffrey (Scott) Calder, MD, USAF, MC
SSG Tommy Chavez, MC, USA
LTC John Chovanes, DO, FACS, MC, USAR
LTC Jason B. Corley, MD, MC, USA
COL Brian Eastridge, MD, MC,USAR
LTC Matthew Eckert, MD, MC, USA
CAPT Ted Edson, MD, MC, USN
CAPT Eric Elster, MD, FACS, MC, USN
Col Mark D. Ervin, FS, USAF, MC
MAJ Colin Frament, PA, MC, USA
COL Tamara Funari, RN, MC, USA
Lt Col Brian J. Gavitt, MD, MPH, FACS, USAF, MC
COL Kirby Robert Gross, MD, MC, USA
Maj Andrew Hall, MD, USAF, MC
LCDR Jonathan Hamrick, USN CRNA, NMCP VA
COL Jason Hiles, MD, MC, USA
MAJ Keith Jackson, MD, MC, USA
SFC Jonathan R. Johnson, ,OPS NCOIC, USA
SMSgt Melissa A. Johnson, USAF, MC
CDR Michel Kearns, MD, MC, USN
Col Peter A. Learn, MD, USAF, MC
MAJ Rich Lesperance MD, MC, USA
Maj Justin D. Manley, FS, USAF, MC
LTC Alex Merkle, USA, PA
CAPT Margaret M. Moore, MD, FACS, MC, USNR
COL Shawn Nessen, MD, MC, USA
SMSgt Jose Arias-Patino, USAF
CDR Travis Polk, MD, FACS, MC, USN
CAPT Robert Ricca, MD, MC, USN
Anne Rizzo MD, FACS
Col James B. Sampson, MD, RPVI, FACS, USAF, MC
COL Martin Schreiber, MD, MC, USAR
COL Jason M. Seery, MD, FACS
CAPT Zsolt Stockinger, MD, MC, USN
CDR Matthew D. Tadlock, MD, FACS, MC, USN
Maj Regina Tai-see, USAF, MC
LTC Eric Verwiebe, MC, USA
COL Paul White, MC, USA
Col Eveline F. Yao, USAF, MC, CFS
References
- The Office of The Surgeon General, Borden Institute. Emergency War Surgery, 5th U.S. Edition, 2018
- Belmont PJ, McCriskin BJ, Hsiao MS, Burks R, Nelson KJ, Schoenfeld AJ. The nature and incidence of musculoskeletal combat wounds in Iraq and Afghanistan (2005-2009). J Orthop Trauma. 2013;27(5):e107-e113. doi:10.1097/BOT.0b013e3182703188.
- Stern CA, Stockinger ZT, Todd WE, Gurney JM. An analysis of orthopedic surgical procedures performed during U.S. combat operations from 2002 to 2016. Mili Med 184.11-12 (2019): 813-819.
- Joint Trauma System, Acute traumatic wound management in the prolonged field care setting CPG. 24 Jul 2017.
- Joint Trauma System, Infection prevention in combat-related injuries CPG. 06 Aug 2016.
- Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg [Am]. 1976;58:453–458.
- Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24:742–746.
- Yun HC, Murray CK, Nelson KJ, Bosse MJ. Infection after orthopaedic trauma: Prevention and treatment. J Orthop Trauma. 2016;30:S21–S26.
- Lack WD, Karunakar MA, Angerame MR, et al. Type III open tibia fractures: immediate antibiotic prophylaxis minimizes infection. J Orthop Trauma. 2015;29:1–6.
- Burns TC, Stinner DJ, Mack AW, et al. Microbiology and injury characteristics in severe open tibia fractures from combat. J Trauma Acute Care Surg. 2012;72(4):1062-1067. doi:10.1097/TA.0b013e318241f534.
- Morgenstern M, Vallejo A, McNally MA, et al. The effect of local antibiotic prophylaxis when treating open limb fractures: a systematic review and meta-analysis. Bone & joint research 7.7 (2018): 447-456.
- Camuso MR. Far-forward fracture stabilization: external fixation versus splinting. J Am Acad Orthop Surg. 2006;14:S118-S123.
- Maury C, Ramin S, Bonfils J, et al. Influence of a temporary stabilization device on respiratory status in patients with severe trauma with a femoral shaft fracture treated by damage control strategy. European Journal of Trauma and Emergency Surgery (2020): 1-12.
- Pape HC, Regel G, Dwenger A, et al. Influence of thoracic trauma and primary femoral intramedullary nailing on the incidence of ARDS in multiple trauma patients. Injury 24 (1993): S82-S103.
- Scalea TM, Boswell SA, Scott JD, et al. External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: damage control orthopedics. J Trauma Acute Care Surg 48.4 (2000): 613-623.
- Blair JA, Kusnezov N, Fisher T, Prabhakar G, Bader JO, Belmont PJ. Early stabilization of femur fractures in the setting of polytrauma is associated with decreased risk of pulmonary complications and mortality. J Surg Orthop Adv. 2019 Summer;28(2):137-143
- Bone LB, Johnson KD, Weigelt J, Scheinberg R. Early versus delayed stabilization of femoral fractures. A prospective. J Bone Joint Surg Am 71 (1989): 336-340.
- Tuttle MS, Smith WR, Williams AE, et al. Safety and efficacy of damage control external fixation versus early definitive stabilization for femoral shaft fractures in the multiple-injured patient. J Trauma Acute Care Surg 67.3 (2009): 602-605.
- Boulanger BR, Stephen D, Brenneman FD. Thoracic trauma and early intramedullary nailing of femur fractures: are we doing harm? J Trauma Acute Care Surg 43.1 (1997): 24-28.
- Possley DR, Burns TC, Stinner DJ, et al. Temporary external fixation is safe in a combat environment. J Trauma. 2010;69:S135-S139.
- Hoppenfeld S. Surgical exposures in orthopaedics: the anatomic approach, 4th ed. Lippincott Williams and Wilkins: Philadelphia, 2009.
- Camathias C, Valderrabano V, Oberli H. Routine pin tract care in external fixation is unnecessary: a randomised, prospective, blinded controlled study. Injury. 2012;43:1969-73.
- Beltran MJ, Collinge CA, Patzkowski JC, et al. The safe zone for external fixator pins in the femur. J Orthop Trauma. 2012;26: 643-647.
Appendix A: Gustilo Classification of Open Fractures
Gustilo Classification of Open Fractures
I Low-energy clean wound <1 cm with minimal soft tissue injury and comminution
II Wound >1 cm with moderate soft tissue damage and comminution. Soft tissue component often defined as disruption <10 cm without periosteal stripping. High-energy wound with skin wound <10 cm involving extensive software tissue destruction, segmental fracture with displacement or bone loss, high degree of contamination, and vascular injury.
IIIa Fracture wound >10 cm with crushed tissue and contamination but usually with adequate soft tissue coverage or any size open wound associated with a segmental fracture (2 or more major fracture lines with intercalary fragment(s)).
IIIb Fracture wound >10 cm with crushed tissue and contamination having inadequate soft tissue cover associated with periosteal stripping and often requiring transfer of rotational or vascularized tissue for soft tissue coverage.
IIIc Open fracture associated with a major vascular injury that requires repair for limb salvage.
Appendix B: Ex-Fix Guide For The Non-Orthopaedic Surgeon
The purpose of an external fixator (“ex-fix”) is to provide a temporizing measure to hold broken bones (usually the femur or tibia) in a reasonable position until further surgery can be performed. The ex-fix provides stability to bones that is particularly important in transfer situations in a combat zone, takes pressure off the surrounding soft tissue and joints, and provides pain relief to the patient.
There are two main types of external fixator constructs:
- Both sets of pins go in the same bone segment.
- Joint-spanning external fixator: one set of pins goes in one bone, and the other set goes into the adjacent bone (e.g. knee-spanning external fixator consists of pins in the femur and the tibia). These are typically performed when the fracture occurs near a joint.
The basic construct consists of the following components:
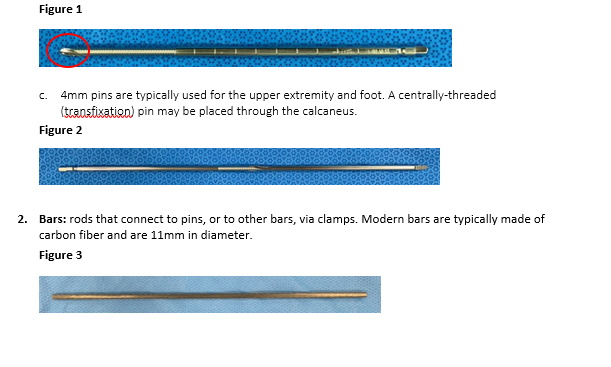
- Pins: stainless steel pins that are drilled into bone, either on power or by hand. The tips of the pins are threaded to prevent them from backing out of bone.
- 5mm pins are typically used for the femur and tibia.
- The drill tip (circled) of the pin should be advanced through the bone to allow full engagement of the threads.
Sterile Field Kit Components
Commercially available sterile field kits allow for placement of an external fixator by hand and typically consist of the following components:
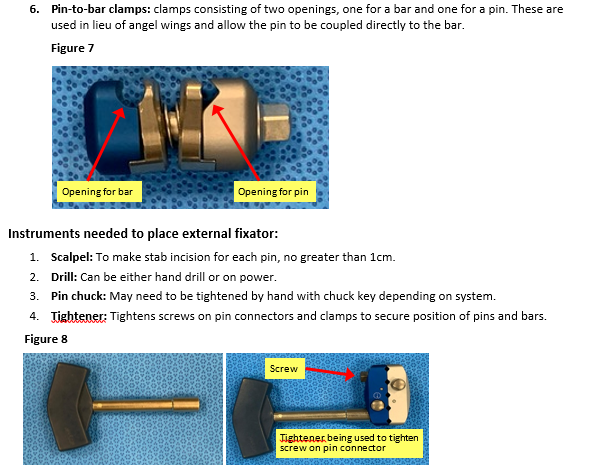
- Scalpel
- Mosquito clamp
- Pins
- Bars
- Manual drill-brace: Serves dual function as hand drill as well as tightener for clamps; each end is labeled for reference (“pin end” and “clamp).
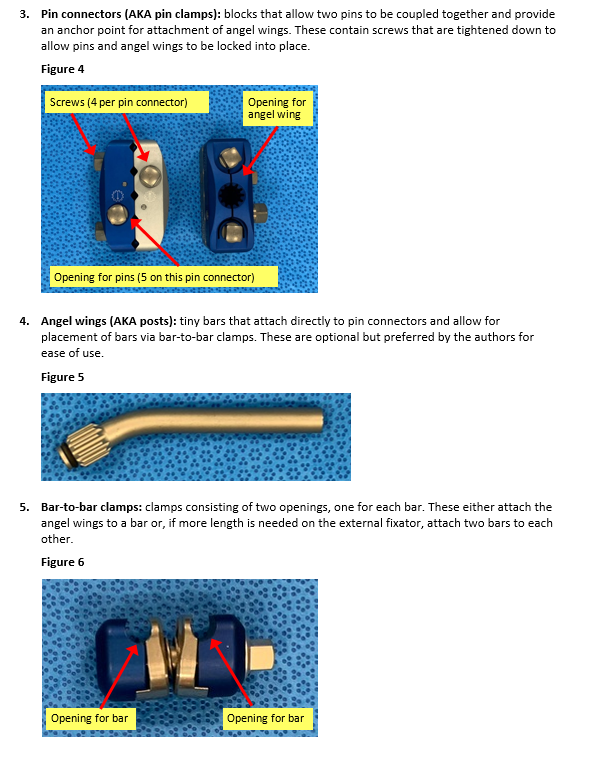
- Bar-to-bar and/or Pin-to-bar clamps
- Pin connectors: Not available in every kit. May come pre-assembled with angel wing.
Basic principles:
- Two pins (at least) are required on each end of the fractured bone.
- Pins should avoid immediate proximity to the fracture site (at least 2-3 fingerbreadths away).
- The external fixator is a tool to reduce fractured bone. Try to restore length and gross alignment.
Minimum Supplies: 4 threaded pins, 2 pin connectors, 2 bars, 2 angel wings (4 suggested), 4 bar-to-bar clamps. Note: Fluoroscopy is beneficial but not essential.
Step-By-Step Instructions (Associated photos for a knee spanning external fixator)
Pin Placement
- Identify external fixator pin sites as described above, taking care to remain in safe zones.
- Femur: Anterior or anterolateral
- Tibia: Just medial to anterior tibial crest (ridge)
- Calcaneus (heel): 1-2 fingerbreadths in front of (anterior) and above (proximal) to the posterior corner of the heel. Drill centrally-threaded pin from medial to lateral to avoid posterior tibial artery.
- Start either proximal or distal to fracture.
- Identify 1st pin site, use scalpel to make stab incision (7-10mm).
- Use a blunt hemostat to dissect down to bone (keep tips of hemostat closed).
- Insert pin perpendicular to bone (Figure 1).
- **Pearl: To drill the tibial pins, it can be helpful to start drilling perpendicular to the bone and create a divot without going all the way through the cortex, then redirect your hand so it is pointing toward the floor. This may help avoid slippage of the drill.
- Place pin bicortically—when using a power drill to insert pins be wary of excessive depth of the pin that can damage deep structures. If inserting by hand and/or without power, once the far cortex is engaged (when increased resistance is felt as the pin is turned), advance the pin an additional 6-8 full turns to reach a safe depth. When fluoroscopic imaging is available, placing pins with power is safe and effective. Hand-inserted pins can be adjusted at follow on facilities when needed.
- If the pin clamps are going to be used, slide pin connector over 1st pin to template location of 2nd pin and mark skin with pin or knife (Figure 2). If clamps are not available or desired, placing the pins in any safe location is possible followed by connection to bars with pin-bar or combination clamps.
- Repeat steps 3-6 for 2nd pin. Placing the pin parallel to the first can reduce the complexity of the fixator, but off-plane pins can increase stability. Pin placement should be decided based on the associated anatomy, fracture and soft tissue injury patterns and fixator stability (Figure 3).
- Move to proximal (or distal) pin site and repeat steps 1-8 (Figure 4).
- Tighten down the screws securing the pins of the proximal and distal pin connectors, ensuring there are 2-3 finger-breaths between the pin connectors and the skin. This is important because swelling will often occur and may lead to skin compromise if the skin is too close to the pin connector. Putting the pin connector too far from the skin, however, will decrease the stability of the construct (Figure 5).
- If fluoroscopy is available, confirm safe, bicortical position of all pins. The drill tip of the pin should be advanced to a depth allowing full engagement of the cortex with the threaded portion of the pin. A few of the threads of the pin should be penetrating through the second cortex.
External fixator Assembly
- Place angel wings onto pin connectors and tighten all components into place with the hand tightener; this includes tightening all screws of the pin connector so that both the pins and the angel wings are secured. (Figure 5)
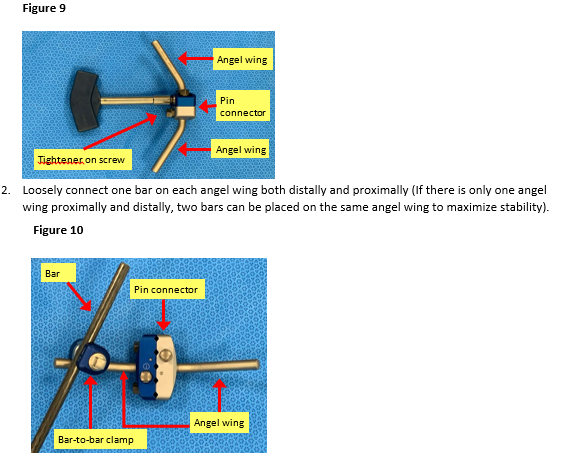
Additional bar(s) may need to be placed on each side and connected to the other bars via bar-to-bar clamps for joint-spanning external fixatores in particular (Figures 6-9).
3. Apply longitudinal traction to restore length and correct the coronal and sagittal alignment of the limb (“make the leg look like a leg”). If fluoroscopy is available, the reduction can be optimized, but an anatomic reduction is not required. Bony apposition improves stability, but can be difficult to maintain with damage control fixators and quickly restoring overall alignment without delaying additional treatment or transfer in the acute phase is preferable.
4.Tighten all components (Figure 6 and Figure 7).
5. Confirm clinical alignment, as well as radiographic alignment if fluoroscopy is available.
6. Dress pins with petroleum gauze (if desired) and Kerlix wrapping between skin and pin connector. (Figure 8 and 9).
Appendix C: Additional Information Regarding Off-Label Uses In CPGS
The purpose of this Appendix is to ensure an understanding of DoD policy and practice regarding inclusion in CPGs of “off-label” uses of U.S. Food and Drug Administration (FDA)–approved products. This applies to off-label uses with patients who are armed forces members.
Unapproved (i.e. “off-label”) uses of FDA-approved products are extremely common in American medicine and are usually not subject to any special regulations. However, under Federal law, in some circumstances, unapproved uses of approved drugs are subject to FDA regulations governing “investigational new drugs.” These circumstances include such uses as part of clinical trials, and in the military context, command required, unapproved uses. Some command requested unapproved uses may also be subject to special regulations.
Additional Information Regarding Off-Label Uses in CPGs
The inclusion in CPGs of off-label uses is not a clinical trial, nor is it a command request or requirement. Further, it does not imply that the Military Health System requires that use by DoD health care practitioners or considers it to be the “standard of care.” Rather, the inclusion in CPGs of off-label uses is to inform the clinical judgment of the responsible health care practitioner by providing information regarding potential risks and benefits of treatment alternatives. The decision is for the clinical judgment of the responsible health care practitioner within the practitioner-patient relationship.
Consistent with this purpose, CPG discussions of off-label uses specifically state that they are uses not approved by the FDA. Further, such discussions are balanced in the presentation of appropriate clinical study data, including any such data that suggest caution in the use of the product and specifically including any FDA-issued warnings.
With respect to such off-label uses, DoD procedure is to maintain a regular system of quality assurance monitoring of outcomes and known potential adverse events. For this reason, the importance of accurate clinical records is underscored.
Good clinical practice includes the provision of appropriate information to patients. Each CPG discussing an unusual off-label use will address the issue of information to patients. When practicable, consideration will be given to including in an appendix an appropriate information sheet for distribution to patients, whether before or after use of the product. Information to patients should address in plain language: a) that the use is not approved by the FDA; b) the reasons why a DoD health care practitioner would decide to use the product for this purpose; and c) the potential risks associated with such use.

