Module 13 - Eye Injuries
Joint Trauma System
Eye Injuries

Tactical Combat Casualty Care is broken up into four roles of care. The most basic is taught to All Service Members (ASM), which is designed to instruct in the absolute basics of hemorrhage control and to recognize more serious injuries.
You are in the Combat Lifesaver (CLS) role. This teaches you more advanced care to treat the most common causes of death on the battlefield, and to recognize, prevent, and communicate with medical personnel the life-threatening complications of these injuries.
The Combat Medic/Corpsman (CMC) role includes much more advanced and invasive care requiring significantly more medical knowledge and skills.
Finally, the last role, Combat Paramedic/Provider (CPP) is for Combat paramedics and advanced providers, to provide the most sophisticated care to keep our wounded warriors alive and get them to definitive care.
Your role as a CLS is to treat the most common causes of death on the battlefield, which are massive hemorrhage and airway/respiratory problems. Also, you are given the skills to prevent complications and treat other associated but not immediately life-threatening injuries.
The eye injury modules has one cognitive learning objective and one performance learning.
The cognitive learning objective is to identify the basic care of an eye injury, and the performance learning objective is to demonstrate the application of a rigid eye shield to a trauma casualty.
The critical aspects are to recognize eye injuries and the steps to treat them, and then to place a rigid eye shield on a trauma casualty.
Remember, you are now in the Tactical Field Care phase of care, and so the focus has shifted from immediate lifethreatening hemorrhage control while still under enemy fire in the Care Under Fire phase, to the reassessment of all previous interventions, followed by the prevention and treatment of other injuries and complications such as head and eye injuries.
Eye injuries are part of the “H” in the MARCH PAWS sequence, as they can be considered head injuries.
Remember, you are now in the Tactical Field Care phase of care, and so the focus has shifted from immediate lifethreatening hemorrhage control while still under enemy fire in the Care Under Fire phase, to the reassessment of all previous interventions, followed by the prevention and treatment of other injuries and complications such as eye injuries.
EYE INJURIES OVERVIEW (VIDEO)
Eyesight is one of our most important senses. Damage to an eye can be irreversible if not treated correctly as early as possible.
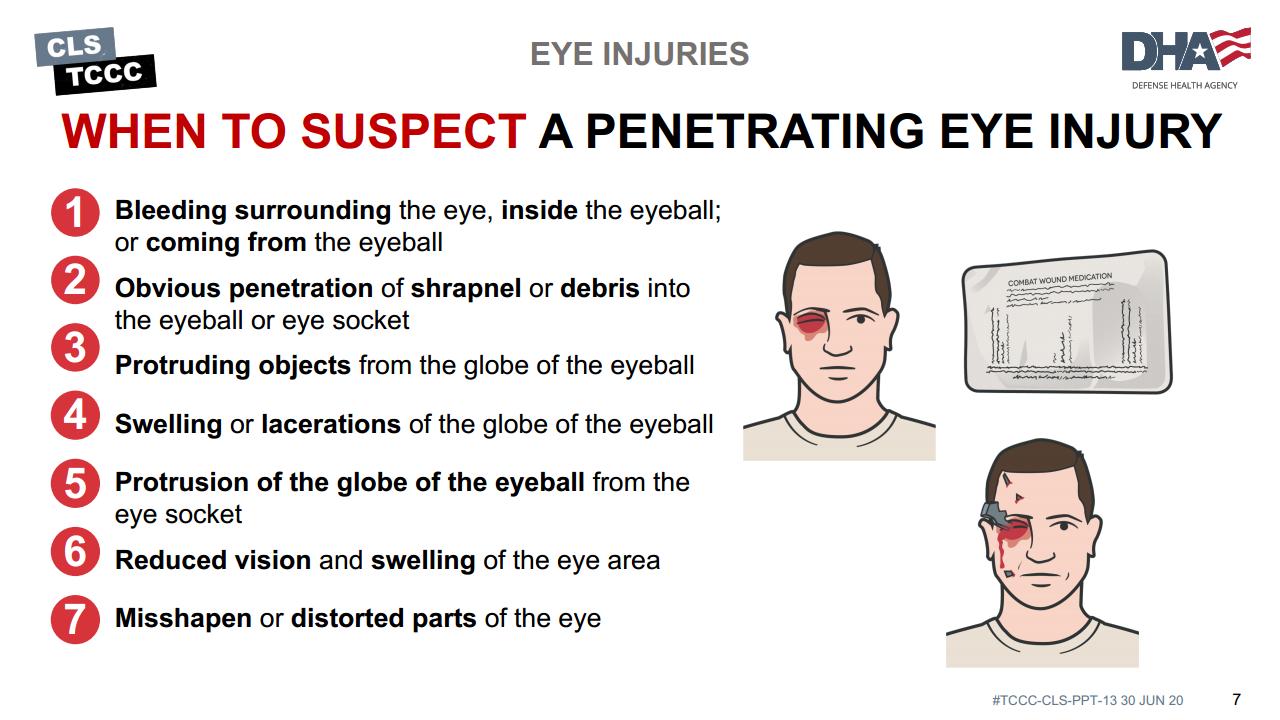
The following signs should make you suspect a penetrating eye injury:
- Bleeding surrounding the eye, inside the eyeball, or coming from the eyeball
- Obvious penetration of shrapnel or debris into the eyeball or eye socket
- Protruding objects from the globe of the eyeball
- Swelling or lacerations of the globe of the eyeball
- Protrusion of the globe of the eyeball from the eye socket
- Reduced vision and swelling of the eye area
- Misshapen or distorted parts of the eye from normal
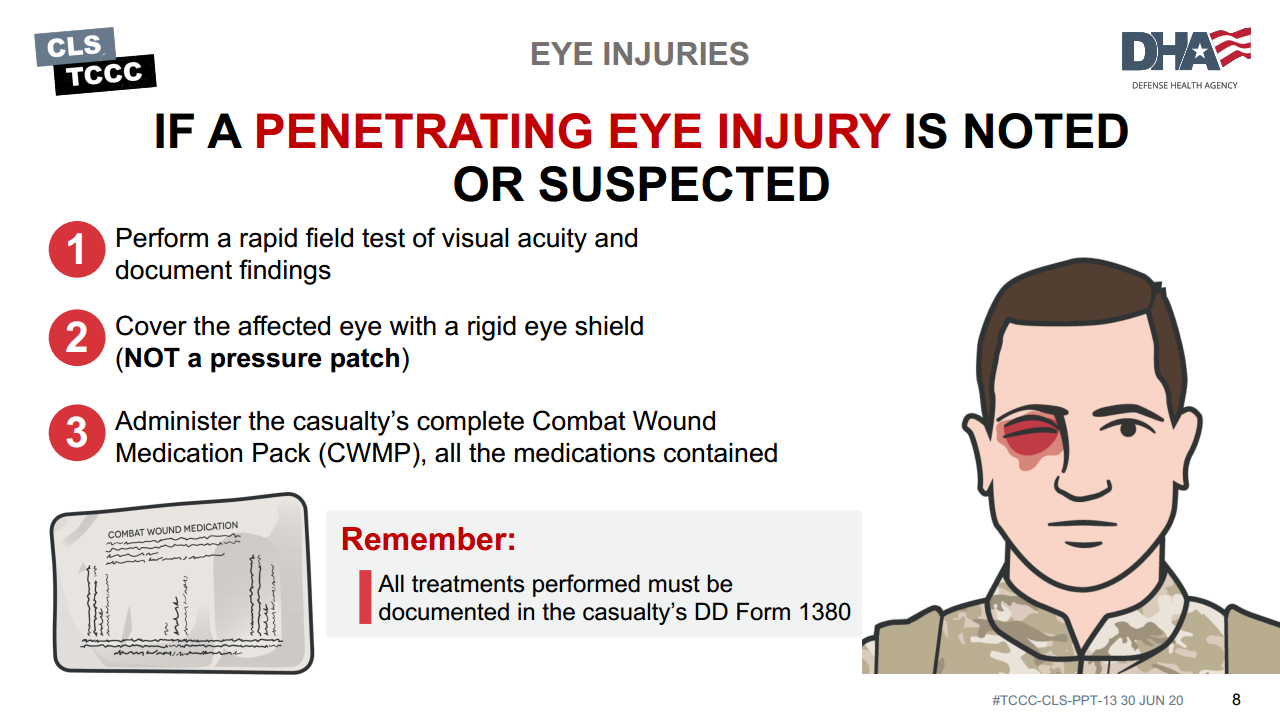
If a penetrating eye injury is noted or suspected, three steps must be taken:
- Perform a rapid field test of visual acuity and document findings
- Rapid visual acuity testing includes the ability to read print, count fingers, identify hand motion, and sense light perception.
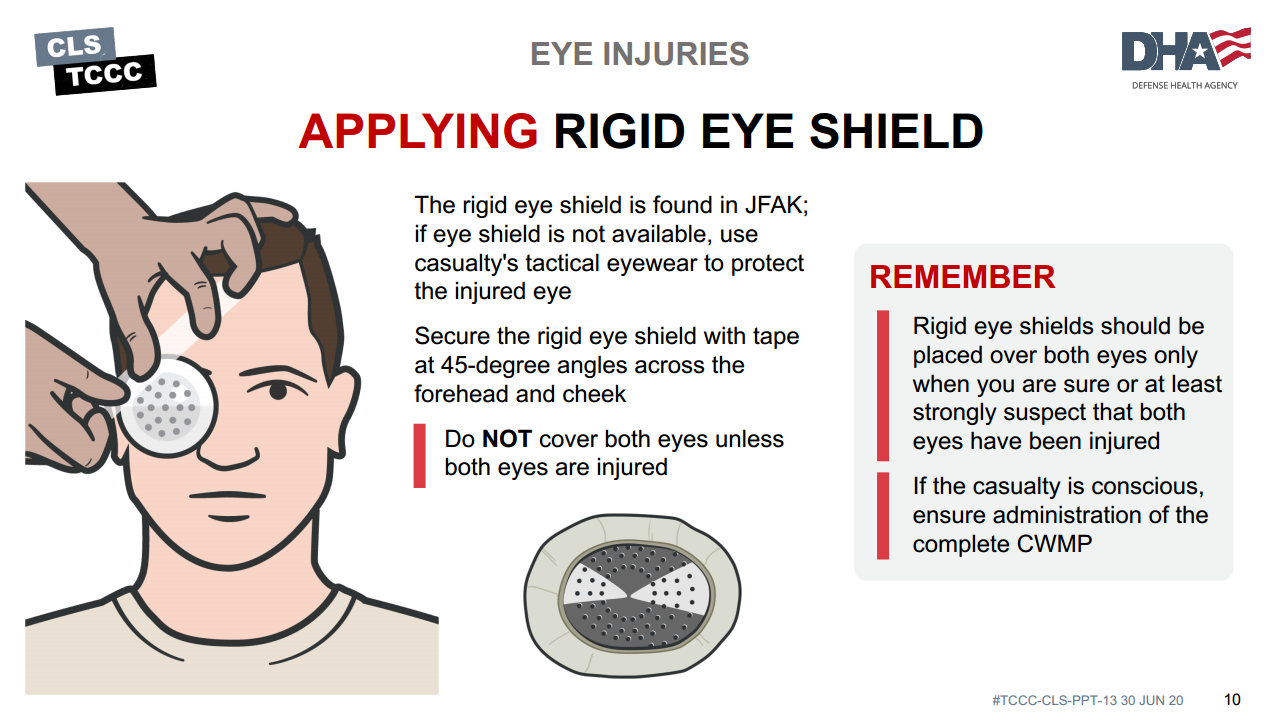
- Cover the affected eye with a rigid eye shield, NOT a pressure patch
- A pressure dressing could result in permanent loss of vision. Place a rigid eye shield on only one eye, unless both eyes are injured. Covering both eyes turns an otherwise ambulatory casualty into a litter casualty. Tactical eyewear is always a good way to prevent eye issues and can be used for protection if no eye shield is available.
- Administer the casualty’s complete Combat Wound Medication Pack (CWMP), including all the medications contained in it.
- One of the medications is 400mg of moxifloxacin, which is administered for eye injuries to prevent infection. Penetrating eye trauma may not always be large injuries from bullets or shrapnel. A cut or laceration of the eye can have the same effect and allow contents to leak from the eyeball. If left untreated, small eye injuries can become infected and cause blindness.
Protect the eye with a SHIELD, not a patch.
A rigid shield will protect the eye from pressure. Avoid/prevent manipulation or additional trauma to the eye that might cause further damage.
Pressure could force the interior contents of the eye to come out of the eyeball.
Pressure dressings are not part of the care of an eye injured in combat and may result in an avoidable permanent loss of vision.
For protruding or impaled objects extending past the eye shield, cut a hole in it to allow the object to fit through, and secure it in place.
If the eye shield cannot be applied around the impaled object, then use an improvised eye shield to avoid pressure on the eye.
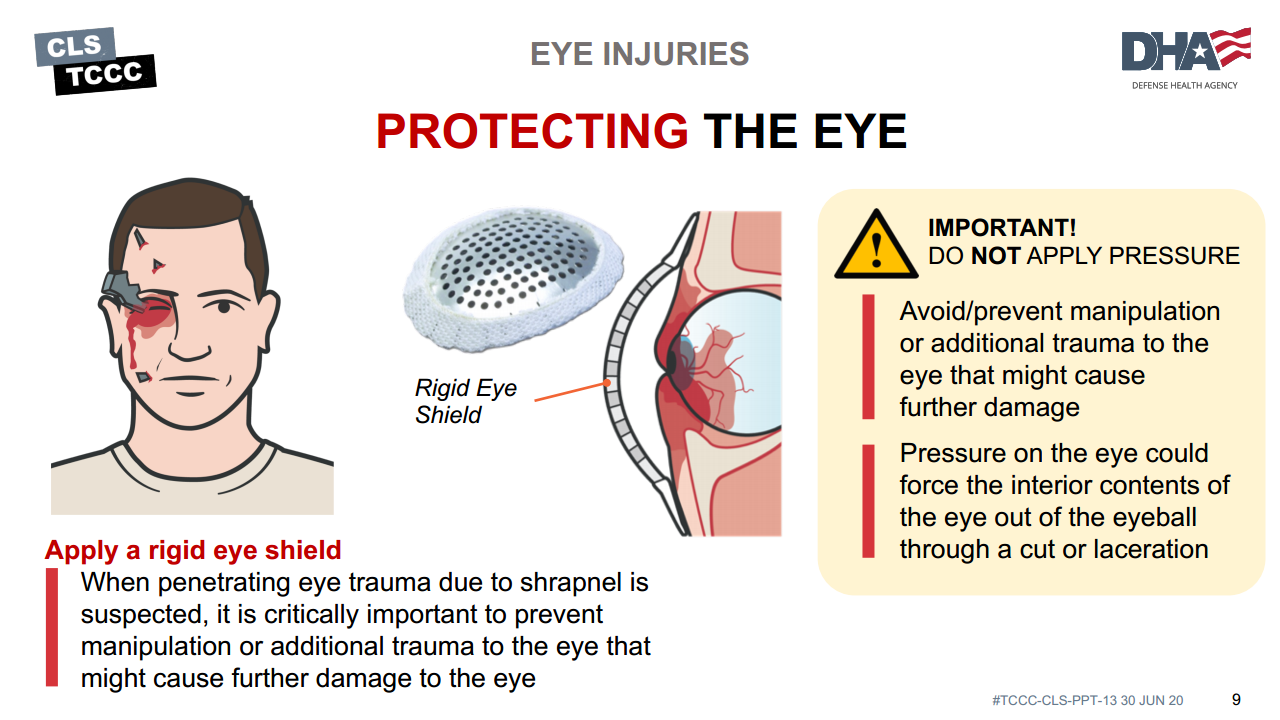
When penetrating eye trauma due to shrapnel is suspected, it is critically important to prevent manipulation or additional trauma to the eye that might cause further damage to the eye.
This is accomplished by taping a rigid shield over the eye. DO NOT apply pressure to the eye.
Secure the rigid eye shield with tape at 45-degree angles across the forehead and cheek.
Rigid eye shields should be placed over both eyes only when you are sure or at least strongly suspect that both eyes have been injured. When only one eye has been injured, do not place a shield over the uninjured eye to prevent eye movement. Movement has not been shown to worsen the outcome for the injured eye. Blindness, resulting from placing eye shields over both eyes unnecessarily, makes an otherwise ambulatory casualty a litter casualty and is psychologically stressful.
If no rigid eye shield is available, tactical eyewear may be used to protect the eyes from further trauma.
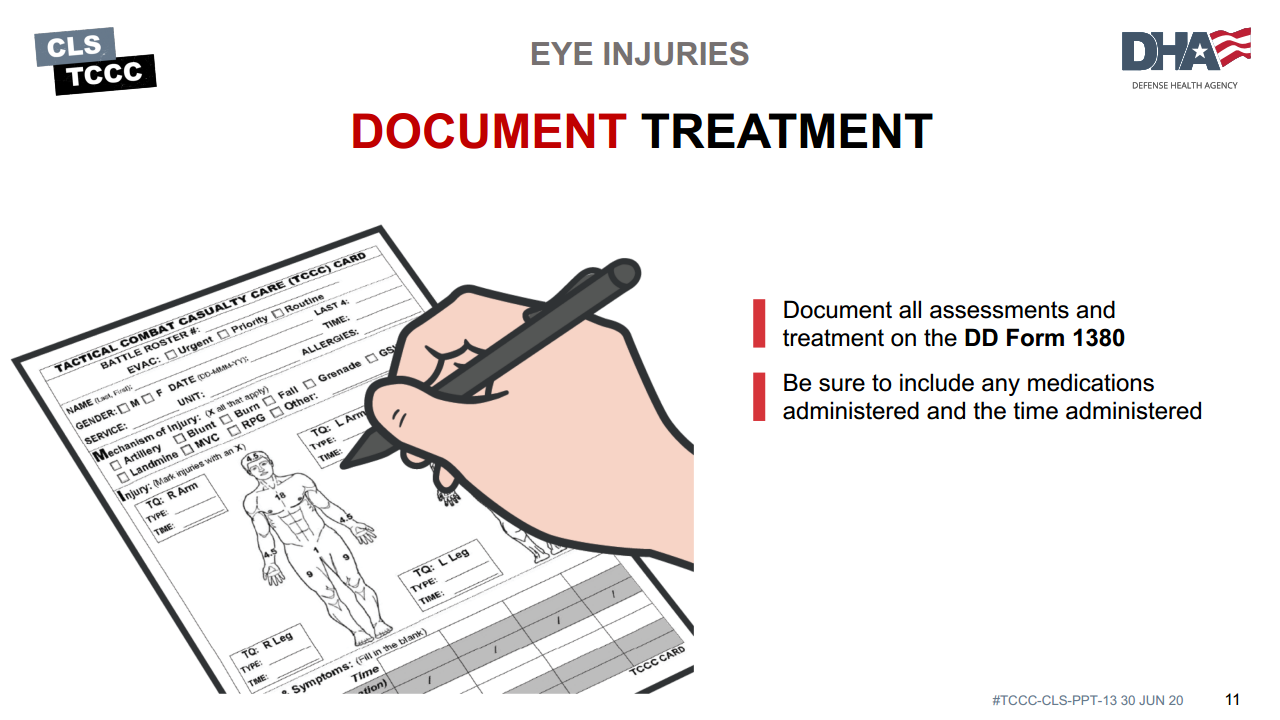
Document all assessments and treatment on the casualty’s DD Form 1380.
Be sure to include any medications administered and the time administered.
APPLYING THE RIGID EYE SHIELD (VIDEO)
At this time we will break into skill stations to practice the following skills:
- Rigid Eye Shield

In this module, we discussed basic care of an eye injury. We addressed how to recognize an eye injury, steps to treat it, application of a rigid eye shield to a trauma casualty, and proper documentation.
To close out this module, check your learning with the questions below (answers under the image).
Answers
What kind of dressing should be used on penetrating eye trauma with an impaled object?
- For protruding/impaled objects extending past the eye shield, cut a hole in it to allow the object to fit through. If you cannot cut the eye shield, place a bulky dressing around the penetrating object.
True or False: Protecting the injured eye with an eye shield is just as safe as using a patch or a pressure dressing?
- False
True or False: Only the injured eye should be covered with an eye shield?
- True