Canine/K9 Tactical Combat Casualty (K9TCCC) Guidelines
K9 Combat Casualty Care Committee
CANINE - TACTICAL COMBAT CASUALTY CARE GUIDELINES
Italicized Text indicates recommendations that are significantly different from human TCCC
BOLD TEXT indicates changes from the 2020 K9TCCC edition
The Joint Trauma System K9TCCC Guidelines are applicable to all Military Working Dogs, Multi-Purpose Canines, Contract Working Dogs or other working dogs that may be present in a deployed or operational environment.
SUMMARY OF 2023 CHANGES
Change the previous MWD and canine terminology references to “K9” to reflect the multiple type of working dogs that may be in a deployed environment. Standardize use of “K9” over “c-” as the official designator for canine products within the Joint Trauma System.
Details or language from the 2019 K9TCCC Guidelines related more to the execution of technical skills have been removed and will be included in the upcoming tiered K9TCCC course packages.
K9TCCC Tactical Field Care:
5. Medication: Addition of Medication consideration between Massive Hemorrhage and Airway Management for K9s.
6. Airway Management: (6d) Previous details or references related to use of mouth gags, laryngoscope and other technical skills for orotracheal/endotracheal intubation have been moved to K9TCCC course packages for further elaboration. Acceptable SpO2 values for intubated K9s on room/atmospheric air has been changed to >90%.
7. Respiration/Breathing: (7a) Anatomic references for localizing the landmarks utilized for needle chest decompression have been moved to the K9TCCC course packages for further elaboration. The catheter/needle combination for NDC should no longer be inserted as a unit to the hub in K9s. Instead, they should be inserted approximately ½ the length of the needle to allow entry into the pleural space and decompression before the catheter is fed off the needle to its hub. (7b) Removed reference to four-sides of adhesive tape for securing a chest seal on a K9 hair coat. Most adherent occlusive chest seals have enough adhesive to stick to the hair coat with better success than tape. Excessive details related to technical skills or clinical knowledge needed for Respiration/Breathing have been moved to the K9TCCC course packages in order to streamline the guidelines.
8. Circulation: (8c) Anatomic locations and technical details for placement of an IV/IO catheter have been moved to the K9TCCC course packages. (8d) Dosing instructions for TXA in a K9 casualty have changed to administering 0.5 gram via slow IV push. (8e) Additions of guidance for the use of calcium supplementation after administration of two K9 blood products. Removal of TBI as a diagnosis and replacement with head injury. (8f) Further clarification is added on who can and where to perform a finger thoracostomy/chest tube insertion.
9. Hypothermia Prevention: Section has been significantly updated to reflect and align with the CoTCCC 2021 TCCC Guidelines language.
12. Analgesia and Sedation/Chemical Restraint: (12a) Meloxicam has been removed for Mild to Moderate Pain. Section has been reorganized into “Mild Pain”, “Moderate to Severe Pain”, and “Chemical Restraint/Sedation” categories for analgesia medications and doses. Ketamine is authorized for Mild Pain and a 50mg dose is listed, while 100mg is reserved for chemical restraint/sedation. Ketamine should be given in combination with either an opioid and/or a benzodiazepine to minimize dissociative effects in K9s. (12b) Updates provided that reflect and align with the CoTCCC 2021 TCCC Guidelines language and the relevant differences between human and K9 patients to consider.
14. Inspect Wounds: (14b) Addition of information for addressing abdominal evisceration.
16. Burns: (16a) Updated guidance on total body surface area estimation based on current K9 specific literature (Henriksson A, et al. 2022). (16e) Hextend has been removed as a recommendation for fluid resuscitation in K9TCCC.
17. Splint Fractures: (17b) Removal of reference to SAM or spoon splints.
18. Cardiopulmonary Resuscitation (CPR): CPR section has been moved up before Communication in alignment with CoTCCC 2021 TCCC Guidelines.
19. Communication: Details regarding S-MIST reporting in K9 casualties has been moved to the K9TCCC course packages for further elaboration.
20. Documentation of Care: (20a) Addition of information regarding DD Form 3073 K9TCCC Card.
21. Prepare for Evacuation: Removal of previous guidance to transport injured K9 requiring emergent surgery to the closest surgical team regardless of if there is a veterinary team in that location. (21e) Refers to staging K9 casualties for evacuation IAW with unit SOPs which should include consideration for location of veterinary assets in the MEDCOP that the K9 can be transported to in relation to concurrent human casualties.
Principles of K9TCCC Tactical Evacuation (TACEVAC):
The K9TCCC Guidelines now include a section on the Basic Management Plan for Tactical Evacuation Care that aligns with the language of the CoTCCC 2021 TCCC Guidelines. Considerations for differences between K9 and human casualties is provided.
6. Head Trauma: (6a, b) Language now includes guidance for Tactical Evacuation Care of head injuries in K9s.
CARE UNDER FIRE
- Return fire and take cover.
- Recall or move the K9 to a safe location if able to maintain positive control. Keep collars and tactical vests on to aid restraint and movement unless causing obvious harm (e.g. choking).
- Apply a muzzle to protect care providers unless respiratory distress or the tactical situation preclude its use. Note: Injured K9s can be unpredictable and harm other team members providing assistance.
- Try to keep the MWD from sustaining additional wounds.
- Injured K9s should be extricated from burning vehicles or buildings and moved to places of relative safety. Do what is necessary to stop the burning process. Remove all burning or smoldering harnesses, collars, vest, booties, goggles, and other gear. Avoid pulling away any items that are melted into the K9’s skin or hair coat; cut hair coat to free melted object.
- Stop life-threatening extremity hemorrhage if tactically feasible:
- Placement of a pressure bandage with or without hemostatic agents.
- Use of CoTCCC-recommended human-designed windlass limb tourniquets are generally ineffective in K9s due to conformational differences and should not be used as first line therapy for hemorrhage control.
- Airway management is generally best deferred until the Tactical Field Care phase.
- Priority for casualty care is given to human combatant casualties before K9 casualties. The handler and K9 should travel together, when appropriate and logistically feasible.
TACTICAL FIELD CARE
Tactical Field Care (TFC) is the care rendered by the first responder or combatant once no longer under effective hostile fire. Tactical Field Care allows more time and a little more safety, to provide further medical care.
1. Establish a Security Perimeter
- Establish a security perimeter in accordance with unit tactical standard operating procedures and/or battle drills. Maintain tactical situational awareness.
2. Triage
- Triage casualties as required. Human casualties should be given priority over K9 casualties.
3. Muzzle
- Muzzle. If not already completed in an earlier phase of care, muzzle when appropriate (not for airway obstruction) to provide safety to personnel handling and treating the K9.
4. Massive Hemorrhage
Assess for unrecognized hemorrhage and control all sources of bleeding with manual or direct pressure via application of hemostatic agents, pressure bandages and/or wound packing as first line intervention. Use kaolin-impregnated bandage (e.g., Combat Gauze) as the CoTCCC hemostatic dressing of choice.
Alternative hemostatic adjuncts:
- Chitosan hemostatic dressing (e.g., Celox™ Gauze or ChitoGauze®) or
- Injectable hemostatic agent (e.g., XStat) best for deep, narrow-tract junctional wounds or
- Hands-free pressure wound sealer (e.g., iTClamp®) may be used alone or in conjunction with hemostatic dressing or injectable hemostatic agent.
Hemostatic dressings should be applied with at least 3 minutes of direct pressure (optional for injectable hemostatic agents). Each dressing works differently, so if one fails to control bleeding, it may be removed and a fresh dressing of the same type or a different type applied. (Note: injectable hemostatic agent is not to be removed in the field, but additional injectable hemostatic agent, other hemostatic adjuncts, or trauma dressings may be applied over it.)
Junctional wounds should be treated with rapid application and packing with hemostatic dressings and direct pressure to control bleeding.
CoTCCC-recommended windlass, limb tourniquets designed for humans (e.g., C-A-T, SOFTT-W) tend to slip distally and fail on K9s due to conformational differences; they should NOT be used as first line therapy for hemorrhage control in K9s.
The only tourniquet that should be considered for use in a K9 with a massive extremity hemorrhage is a stretchable and elastic tourniquet such as the SWAT-T. The material type and wide design allow it to mold to any limb size or conformation and serve as an effective circumferential pressure bandage on a K9’s limb.
Junctional tourniquets have not been evaluated in K9s and are not recommended at this time.
Perform initial assessment for hemorrhagic shock and consider immediate initiation for shock resuscitation efforts.
5. Medication
- K9 may need sedation or pain management to provide treatment. See Section 12.
6. Airway Management
Conscious K9 with no airway problems identified:
- No airway interventions needed.
Unconscious K9 without airway obstruction:
Perform basic airway maneuvers:
Extend the head and neck into a straight in-line position.
Grasp the tongue, gently extend it out of the mouth, and pull it down over the lower jaw.
Consider endotracheal intubation to achieve/maintain patent airway if progression of clinical signs warrant (refer to 6d).
Consider using a mouth gag to keep the K9’s mouth open and prevent damage to endotracheal tube.
K9 with airway obstruction or impending airway obstruction:
Allow a conscious K9 to assume any position that best allows it to breathe with minimal restriction of air flow and protects the airway (position of comfort), to include sitting or standing.
Place an unconscious K9 in the recovery position.
Palpate throat (pharyngeal area, larynx, and trachea) to identify any abnormal mass or foreign material.
Open mouth to examine oropharyngeal area:
Avoid placing hands or fingers directly in the K9’s mouth.
Consider using a leash, rope or roll gauze looped behind the upper and lower K9 teeth to hold the K9’s mouth open.
Consider sedating the K9 (see Section 12 below).
Use suction to clear airway if available, appropriate and feasible based upon K9 disposition/mental status.
If the previous measures are unsuccessful to clear or remove the airway obstruction, or the K9 collapses or becomes unconscious consider one of the following techniques. All K9 airway support requires continuous patient monitoring and care:
Orotracheal Intubation (OTI) / Endotracheal Intubation (ETI):
If the necessary equipment is available, the preferred technique for gaining airway access in an unconscious or anesthetized K9 without oral trauma based on resources available and expected evacuation time. With training this can be accomplished in field conditions.
K9 needs to be maintained at a surgical plane of anesthesia.
Intubation is most easily performed in sternal or lateral with head and neck extended with tongue pulled forward.
Use largest available tube up to 10.0 mm internal diameter, with or without laryngoscopy.
If previous measures are not feasible, unsuccessful, or if the K9 regains consciousness and cannot be maintained under anesthesia, perform a surgical airway based on skills, experience, proficiency and authorizations of the treating medical provider.

Figure 2. Position MWD for intubation

Figure 3. Place tip of laryngoscope blade on back of tongue
DO NOT TOUCH THE EPIGLOTTIS (triangular tissue guarding the opening of the trachea)

Figure 4. Push downward with the laryngoscope blade to move the epiglottis and visualize the trachea

Figure 5. Using a slight side to side motion, guide the endotracheal tube over the epiglottis between the vocal cords

Figure 6. Advance and secure endotracheal tube
Advance the endotracheal tube into the trachea until your marked spot is even with the canine teeth.
Secure tube by placing attached roll gauze behind canine teeth and tying the loose ends in a bow around the upper or lower jaw.

Figure 7. Check for proper placement.
One tube= In the trachea
Two tubes= In the esophagus

Figure 8. Inflate the cuff with a syringe until back pressure is noted

Surgical Airways
Surgical Cricothyrotomy (CTT)
Use techniques recommended for humans.
Bougie-aided open surgical, flanged and cuffed airway cannula, with largest diameter tube available up to 8mm internal diameter.
Standard open surgical, flanged and cuffed airway cannula, with largest diameter tube available up to 8mm internal diameter.
Surgical Tube Tracheostomy (STT)
Use the largest internal diameter that fits into K9 trachea; aim for a TT that is at least 70% of the estimated internal tracheal lumen diameter.
Select a TT length of 5-8cm or one that does not extend beyond the thoracic inlet/point of the shoulder.
Blind Insertion Airway Device / Nasopharyngeal airways / Extraglottic Airway Devices should NOT be utilized in K9s due to their anatomy.
K9s possess a proportionally larger tracheal lumen diameter as compared to humans.
If necessary, assisted ventilation via a bag valve mask (BVM) device can be performed at a rate of 8-10 breaths per minute with the mask portion removed.
Figure 9. Position MWD on its back
Extend the neck and place something under it to force it upwards, making it easier to visualize the trachea.

Figure 10. Make a full thickness skin incision along the center of the neck 2-3 finger widths below the larynx (voice box)using a scalpel blade.
If obstruction is in the trachea you must use a lower spot; otherwise use landmarks given.
Do NOT make a transverse skin incision (perpendicular to the long axis of the trachea), as this increases the risk of injury to adjacent vessels and nerves.

Figure 11. Use a scalpel to carefully separate the muscles the run parallel to the incision.

Figure 12. Hold the muscles apart to visualize the trachea

Figure 13. Make an incision in the trachea.
Stabilize the trachea with non-dominant hand
Make an incision between two rings of the trachea (between the 3rd and 4th or 4th and 5th tracheal cartilages). Do NOT extend the incision more than one-half (50%) of the diameter of the trachea. Do NOT incise at the cricothyroid ligament, as is done in people.
Remove blood or mucus, if present.

Figure 14. Insert the tracheal retractor into the trachea

Figure 15. Hook a lower tracheal ring and lift up so you can visualize the tracheal opening

Figure 16. Insert tracheostomy tube (ideal) or endotracheal tube through the incision and direct the distal opening down the trachea.
Use the largest tube that will fit in the trachea; (7-11mm internal diameter tubes are typical).

Figure 17. Immediately provide supplemental oxygen
Breathe in the tube or use a hand-operated resuscitator

Figure 18. Secure the tracheal tube
Secure the tracheal tube by attaching gauze bandage to the tube and tying it around the dog’s neck in a bow knot. Inflate the cuff until you get back pressure.
If using a tracheostomy tube, secure the tracheostomy tube to the patient using umbilical tape, roll gauze, or similar material tied to the wings of the tube and passed around the neck and tied with a quick release knot. Insert the inner cannula (if provided) in the tracheostomy tube (if used) and inflate the cuff of the tracheostomy tube.

Cervical spine stabilization in the K9 casualty is difficult to achieve in a tactical environment and not required.
Monitor capnography (End Tidal CO2) and pulse oximetry (SpO2) in K9s when available to help assess airway patency.
Capnography setup and values for K9s is the same as for humans.
Normal SpO2 values in K9s are similar to those in humans (> 90% on room / atmospheric air). Pulse Oximetry probe placement for K9s in order of preference: tongue, non-pigmented area of lip, ear pinna, prepuce (male) or vulva (female).
Always remember that the K9’s airway status may change over time and requires continuous reassessment.
Airway Notes:
Consider a K9 that is barking, growling, or whining without any clinical signs of respiratory distress to have a patent airway. This is similar to a human casualty that can speak clearly without any respiratory distress.
Consider monitoring K9 rectal temperature for hyperthermia related to upper airway obstruction or hypothermia due to shock.
7. Respiration/ Breathing
- Assess for tension pneumothorax and treat, as necessary.
- Suspect a tension pneumothorax and treat when a casualty has significant torso trauma or primary blast injury and one or more of the following:
- Severe or progressive respiratory distress
- Severe or progressive tachypnea
- Absent or markedly decreased breath sounds on one side of the chest
- Rapid, shallow, restrictive and open-mouth breathing
- Hemoglobin oxygen saturation <90% on pulse oximetry
- Shock
- Traumatic cardiac arrest without obviously fatal wounds
- If not treated promptly, tension pneumothorax may progress from respiratory distress to shock and traumatic cardiac arrest.
- Suspect a tension pneumothorax and treat when a casualty has significant torso trauma or primary blast injury and one or more of the following:
Figure 19. Apply occlusive seal to wound

Figure 20. Seal the occlusive dressing by applying pressure

Figure 21. Dress the wound
Maintain pressure on occlusive seal.
With free hand, place dressing over occlusive seal.
Use free ends of dressing to bandage around chest.
If the air tight seal is lost at any time during this process, start over.

Figure 22. Apply bandage of non-adherent conforming material over the field dressing to add security

- Initial treatment of suspected tension pneumothorax:
- If the casualty has a chest seal in place, burp or remove the chest seal.
- Allow a conscious K9 to assume the position of comfort. If unconscious, place casualty in recovery position or lateral recumbency with the injured/affected side facing up.
- Decompress the chest on the side of the injury with a 14-gauge or a 10-gauge, 3.25-inch needle/catheter unit (chest needle decompression (NDC)).
- The 7th-9th intercostal space (ICS) either midway up the lateral thoracic wall OR at the junctions of the upper 1/3rd and lower 2/3rd of the thoracic wall may be used for decompression (NDC).
- The needle/catheter unit should be inserted at an angle perpendicular to the chest wall and just over the front of the rib (toward the K9’s head) at the insertion site. Insert the needle/catheter unit together until the needle can be felt entering the pleural space (this occurs when the catheter is inserted approximately ½ of its length) and hold it in place for 5-10 seconds to allow decompression to occur. Do not insert the needle/catheter unit all the way to the hub due to significant differences in K9 anatomy.
- After the NDC has been performed, feed the catheter the rest of the way into the pleural cavity, remove the needle, and leave the catheter in place. If a casualty has significant torso trauma or primary blast injury and is in traumatic cardiac arrest (no pulse, no respirations, no response to painful stimuli, no other signs of life), decompress both sides of the chest before discontinuing treatment.
- Establish pulse oximetry monitoring if available.
- The NDC should be considered successful if:
- Respiratory distress improves, or
- There is an obvious hissing sound as air escapes from the chest when NDC is performed (this may be difficult to appreciate in high-noise environments), or
- Hemoglobin oxygen saturation increases to 90% or greater (note that this may take several minutes and may not happen at altitude), or
- A casualty with no vital signs has return of unconsciousness and/or femoral pulse.
- Consider decompressing BOTH SIDES (LEFT & RIGHT) of the chest, particularly if decompression of the initial side fails to fully relieve signs consistent with a tension pneumothorax due to the differences in K9 anatomy.
- If the initial NDC fails to improve the K9 casualty’s signs/symptoms from the suspected tension pneumothorax:
- If the K9 casualty was in sternal recumbency, reposition into lateral recumbency and perform a second NDC on the same side of the chest. Use a new needle/catheter unit for the second attempt.
- Reposition the K9 and perform a NDC on the opposite chest wall using a new needle/catheter unit.
- Consider, based on the mechanism of injury and physical findings, whether decompression of the opposite side of the chest may be needed.
- Continue to reassess!
- If the initial NDC was successful, but symptoms later recur:
- Perform another NDC at the same site that was used previously. Use a new needle/catheter unit for the repeat NDC.
- Continue to reassess!
- If the second NDC is also not successful:
- Continue on to the Circulation section of the K9TCCC Guidelines.
All open and/or sucking chest wounds should be treated by immediately applying a vented chest seal to cover the defect. If a vented chest seal is not available, use a non-vented chest seal. Monitor the K9 for the potential development of a subsequent tension pneumothorax. If the K9 develops increasing hypoxia, respiratory distress, or hypotension and a tension pneumothorax is suspected, treat by burping or removing the dressing or by needle decompression.
K9 hair coats limit the ability to achieve an occlusive seal and may require additional measures including use of petroleum impregnated gauze under the chest seal or a loosely placed circumferential chest wrap.
Initiate pulse oximetry. All K9s with moderate/severe head injury should be monitored with pulse oximetry. Readings may be misleading in the settings of shock or marked hypothermia.
K9s with a head injury should be given supplemental oxygen when available to maintain an oxygen saturation > 90%.
8. Circulation
Bleeding
Reassess sites of major hemorrhage and associated hemostatic interventions. If bleeding persists, consider changing or adding additional hemostatic adjuncts (e.g., Combat Gauze, chitosan-based dressings, or X-Stat) and/or reapplying circumferential pressure bandages and wound packing, and/or applying a wide elastic tourniquet (e.g., SWAT-T) where applicable.
Hands-free pressure wound sealer (e.g., iTClamp) should be considered to close bleeding open wounds or can be used concurrently with hemostatic agents.
Pelvic binders are not recommended in K9s at this time.
Expose and clearly mark all tourniquets if they were applied with the time of tourniquet application. Note tourniquets applied and time of application; time of reapplication; time of conversion; and time of removal on the K9TCCC Casualty Card (DD 3073). Use a permanent marker to mark on the tourniquet and the casualty card.
Assess for hemorrhagic shock (pale mucous membranes, inappropriate mentation in the absence of head trauma and/or weak or absent femoral pulse).
IV/IO Access
Intravenous (IV) or intraosseous (IO) access is indicated if the K9 is in hemorrhagic shock or at a significant risk of shock (and may therefore need fluid resuscitation), or if the K9 needs injectable medications.
An 18-gauge IV or saline lock is preferred.
If vascular access is needed but not quickly obtainable via the IV route, use the IO route.
Figure 23. Position the dog
Muzzle the dog. Handler restrains the dog in a sitting position or lying on its chest. If dog is conscious, handler restrains the dog's head by wrapping the arm around the dog's neck and cradling the dog's head and neck in the elbow.

Figure 24. Occlude the cephalic vein
If dog is conscious, handler places thumb over the cephalic vein and heel of the hand under the dog's elbow. If dog is unconscious, can use a tourniquet. Extend the arm at the elbow.

Figure 25. Placing your thumb directly besides the vein and wrapping your remaining fingers underneath the leg, pierce the skin with the catheter needle
Bevel facing up at a 10 to 30 degree angle to the skin
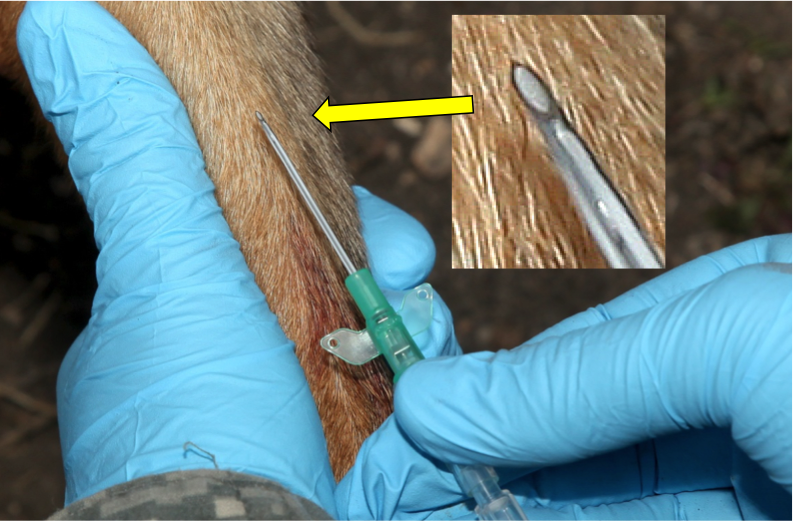
Figure 26. Pierce the vein by advancing the catheter and then decrease the angle of the catheter until almost parrallel to the skin surface.
The flash of blood confirms correct placement.

Figure 27. Advance the catheter needle approximately 1/4 inch into the vein using a gentle forward motion

Figure 28. Advance the catheter into the vein as far as possible while holding the catheter needle hub with one hand
Then have the handler release pressure on the vein but continue to hold elbow in place; or release tourniquet.

Figure 29. Remove the needle from the catheter by pulling it out while stabilizing the catheter
Then quickly attach catheter injection port onto the hub of the catheter.

Figure 30. Secure the catheter to the limb with tape

Figure 31. Location for IO catheter placement on proximal medial tibia

Figure 32. Intended insertion site (red oval) on proximal medial tibial crest, just distal to the knee joint

Figure 33. Insertion of pediatric IO catheter in proximomedial tibia using EZ-IO device

Figure 34. Full insertion of IO catheter after removal of stylet

Tranexamic Acid (TXA)
- If a K9 is anticipated to need significant blood transfusion (e.g., presents with hemorrhagic shock, one or more major amputations, penetrating torso or abdominal trauma, or evidence of severe bleeding):
OR
- If the K9 has signs or symptoms of significant head injury or has altered mental status associated with blast injury or blunt trauma:
- Administer 0.5 gram of TXA by slow IV push as soon as possible but NOT later than 3 hours after injury.
Fluid resuscitation
- Assess for hemorrhagic shock (pale mucus membranes, inappropriate mentation in the absence of head trauma, weak or absent femoral pulse).
- The resuscitation fluids of choice for K9s in hemorrhagic shock, listed from most to least preferred, are:
1. K9 chilled or fresh whole blood
2. K9 plasma and RBCs in a 1:1 ratio
3. K9 plasma or RBCs alone
4. Crystalloid (Lactated Ringer’s, Normosol R or Plasma-Lyte A)
NOTE: Hypothermia preventions measures [Section 9] should be initiated while fluid resuscitation is being accomplished
NOTE: DO NOT administer human blood products to a K9 due to a high risk of transfusion reaction.
- If not in shock:
- NO IV fluids are immediately necessary.
- Fluids by mouth are permissible if the K9 is conscious and can swallow.
- If in shock and K9 blood products are available under an approved command or theater blood product administration protocol:
- Resuscitate with K9 whole blood or, if not available
- K9 plasma and K9 pRBCs in a 1:1 ratio, or if not available
- Reconstituted lyophilized K9 plasma, K9 liquid plasma or thawed K9 fresh frozen plasma alone or K9 pRBCs alone. A second unit may be required.
- Reassess the K9 after each unit. Continue resuscitation until a palpable femoral pulse, improved mental status or systolic BP of 100-110 mmHg is present.
- Discontinue fluid administration when one or more of the above end points have been reached.
- If blood products are transfused, administer one gram of calcium IV/IO after the second transfused product.
- Transfusion should occur as soon as possible after life-threatening hemorrhage in order to keep the patient alive.
- Given increased risk for potentially lethal hemolytic reaction in K9s that have received previous transfusion therapy >72 hours prior to injury, they should only receive a transfusion under appropriate medical direction by a veterinarian.
- If in shock and blood products are not available due to tactical or logistical constraints
- Lactated Ringer’s or other buffered crystalloid solution.
- Reassess the K9 after each IV/IO bolus.
- Continue resuscitation until a palpable femoral pulse, improved mental status, or systolic BP of 100-110 mmHg is present.
- If a K9 with an altered inappropriate mentation due to suspected head injury has a weak or absent femoral pulse, resuscitate as necessary to restore and maintain a normal femoral pulse. If BP monitoring is available, maintain a target systolic BP of at least 100-110 mmHg.
- Reassess the K9 frequently to check for recurrence of shock. If shock recurs, re-check all external hemorrhage control measures to ensure that they are still effective and repeat the fluid resuscitation as outlined above.
Refractory Shock
- If a K9 casualty in shock is not responding to fluid resuscitation, consider untreated tension pneumothorax as a possible cause of refractory shock.
- Thoracic trauma, persistent respiratory distress, absent breath sounds, and hemoglobin oxygen saturation < 90% support this diagnosis.
- Treat as indicated above with repeated NDC or finger thoracostomy/chest tube insertion at the 7th-9th intercostal space, according to the skills, experience, and authorizations of the treating medical provider.
- Note that if finger thoracostomy is used, it may not remain patent and finger decompression through the incision may have to be repeated. Consider decompressing the opposite side of the chest if indicated based on the mechanism of injury and physical findings.
9. Hypothermia Prevention
- Take early and aggressive steps to prevent further body heat loss and add external heat when possible for both trauma and severely burned casualties.
- Minimize K9 casualty’s exposure to cold ground, wind and air temperatures. Place insulation material between the K9 casualty and any cold surface as soon as possible.
- Remove any wet outer wear (e.g., vests, harnesses, booties, etc.). GENTLY pat dry any wet tissues or hair coat.
- Place an active heating blanket on the K9 casualty’s torso (to prevent burns, do not place any active heating source directly on the haired skin or wrap around the torso).
- Enclose the K9 casualty with the exterior impermeable enclosure bag.
- As soon as possible, upgrade hypothermia enclosure system to a well-insulated enclosure system using a hooded sleeping bag or other readily available insulation inside the enclosure bag/external vapor barrier shell.
- Pre-stage an insulated hypothermia enclosure system with external active heating for transition from the non-insulated hypothermia enclosure systems; seek to improve upon existing enclosure system when possible.
- Use a battery-powered warming device to deliver IV/IO resuscitation fluids, in accordance with current K9TCCC guidelines, if IV fluids are required.
- Protect the K9 casualty from exposure to wind and precipitation on any evacuation platform
10. Penetrating Eye Trauma
- If a penetrating eye injury is noted or suspected:
- Place muzzle if practical before examining the eye.
- Do NOT attempt to bandage or cover the eye. Make every effort to prevent K9. from scratching at the eye. Consider sedation as outlined in Section 12.
- If possible, gently rinse the eye with clean water.
- Ensure that oral or IV/IM antibiotics are given as outlined below.
- Ketamine can cause nystagmus and increase intraocular pressure in a K9. Consider alternative sedatives/analgesics in K9s with penetrating eye trauma unless other alternatives do not exist or are ineffective.
11. Monitoring
- Initiate advanced electronic monitoring if indicated and if monitoring equipment is available.
12. Analgesia and Sedation/Chemical Restraint
Analgesia on the battlefield should generally be achieved using one of three options:
TCCC Medical and Veterinary Personnel should provide analgesia on the battlefield based on K9 casualty status using the following drugs listed:
Mild Pain:
Opioid alone (if the K9 is not fractious, an opioid may be all that is needed)
Morphine at 0.25-0.5mg/kg IM (equivalent to one 10mg morphine autoinjector) or
Hydromorphone 0.1 mg/kg IV/IO/IM or
Fentanyl (injectable) every 20-30 minutes at 2-5mcg/kg IV/IO or 10mcg/kg IM
Ketamine (50mg) IV/IM/IO + Midazolam (10mg) IV/IO/IM
Moderate to Severe Pain:
Ketamine (50mg) IV/IM/IO + Opioid
Morphine at 0.25-0.5 mg/kg IM (equivalent to one 10mg morphine autoinjector) or
Hydromorphone 0.1 mg/kg IV/IO/IM or
Fentanyl (injectable) every 20-30 minutes at 2-5 mcg/kg IV/IO or 10 mcg/kg IM
Ketamine (50mg) IV/IM/IO + Midazolam (10mg) IV/IO/IM + Opioid
Morphine at 0.25-0.5 mg/kg IM (equivalent to one 10mg morphine autoinjector) or
Hydromorphone 0.1 mg/kg IV/IO/IM or
Fentanyl (injectable) every 20-30 minutes at 2-5 mcg/kg IV/IO or 10 mcg/kg IM
Chemical Restraint/Sedation:
Ketamine (100 mg) IV/IM/IO + Midazolam (10mg) IV/IO/IM or
Ketamine(100 mg) IV/IM/IO + Opioid.
Morphine at 0.25-05 mg/kg IM (equivalent to one 10mg morphine autoinjector) or
Hydromorphone 0.1mg/kg IV/IO/IM or
Fentanyl (injectable) every 20-30 minutes at 2-5 mcg/kg IV/IO or 10 mcg/kg IM
Analgesia and sedation/chemical restraint notes:
- The goal of analgesia is to reduce pain to a tolerable level while still protecting K9 airway and mentation.
- The goal of sedation/chemical restraint is to stop awareness of painful procedures and prevent injury to medical personnel.
- For all K9s given opioids, ketamine or benzodiazepines – closely monitor airway, breathing, and circulation.
- DO NOT administer Oral Transmucosal Fentanyl Citrate (OFTC) to a K9 orally or per rectum.
- Naloxone should be available when using opioid analgesics.
- Recommended doses are: 2mg IV/IO or 4mg IM/IN. Repeat as needed.
- Opioid doses for K9s are significantly higher than humans and often cause vomiting so handlers and medics should be prepared to remove the muzzle after administration of an opioid.
- Hydromorphone causes excessive panting; use caution with head injuries and respiratory disease.
- Head injury and/or non-penetrating eye injury does not preclude the use of ketamine in K9s at the K9TCCC recommended doses. Use caution with IV/IO ketamine, or midazolam in a head injury as this makes it difficult to perform a neurological exam or determine if the casualty is decompensating.
- The sole use of routine benzodiazepines such as midazolam is NOT recommended for analgesia.
- If a K9 appears to be partially dissociated, it is more efficacious to administer more ketamine than to administer more benzodiazepine.
- Polypharmacy is recommended in K9s; benzodiazepines can be used in conjunction with ketamine and/or opioid analgesia.
13. Antibiotics
- Antibiotics are recommended for all open combat wounds.
- Recommended antibiotics are:
- Ceftriaxone 25 mg/kg IV/IM q 12 hours
- Cefotaxime 25 mg/kg IV/IM q 8 hours
- Ertapenem 15-30 mg/kg IV/SC every 8 hours
- If able to take PO meds consider:
- Moxifloxacin 400 mg PO once a day
14. Inspect Wounds
- Inspect and dress known wounds.
- Abdominal evisceration – [Control bleeding]: rinse with clean (and warm if possible) fluid to reduce gross contamination. Hemorrhage control – apply combat gauze or CoTCCC recommended hemostatic dressing to uncontrolled bleeding. Cover exposed bowel with a moist, sterile dressing or sterile water-impermeable covering.
- Reduction: do not attempt if there is evidence of ruptured bowel (gastric/intestinal fluid or stool leakage) or active bleeding.
- If no evidence of bowel leakage and hemorrhage is visibly controlled, a single brief attempt (<60 seconds) may be made to replace/reduce the eviscerated abdominal contents.
- If unable to reduce; cover the eviscerated organs with water impermeable non-adhesive material (transparent preferred to allow ability to reassess for ongoing bleeding); examples include a bowel bag, IV bag, clear food wrap, etc. and secure the impermeable dressing to the patient using adhesive dressing (examples: ioban, chest seal)
- DO NOT FORCE contents or actively bleeding viscera back into abdomen.
- The patient should remain NPO.
15. Check for Additional Wounds
Check for additional wounds.
16. Burns
- Assess and treat as a K9 trauma casualty with burns and not a burn casualty with injuries.
- Facial burns, especially those that occur in closed spaces, may be associated with inhalation injury. Aggressively monitor airway status and oxygen saturation in such K9 patients and consider early intubation or surgical airway for respiratory distress or oxygen desaturation.
- Estimate total body surface area (TBSA) burned to the nearest 10% using the published chart (Henriksson A, et al. 2022) for estimating canine body surface area, similar to human Rule of Nines.
- Cover the burn area with dry, sterile dressings. For extensive burns (>20%), consider placing the K9 casualty in the Heat-Reflective Shell or Blizzard Survival Blanket from the Hypothermia Prevention Kit in order to both cover the burned areas and prevent hypothermia.
- Fluid resuscitation (extrapolated from the U.S. Army Institute of Surgical Research Rule of Ten).
- If burns are greater than 20% of TBSA, fluid resuscitation should be initiated as soon as IV/IO access is established. Initiate resuscitation with (order of preference) Lactated Ringer’s, Plasma-Lyte A/Normosol-R, or normal saline.
- Initial IV/IO fluid rate is calculated as %TBSA x 10 ml/hr
- If hemorrhagic shock is also present, resuscitation for hemorrhagic shock takes precedence over resuscitation for burn shock. Administer IV/IO fluids per the K9TCCC Guidelines in Section 8.
- If burns are greater than 20% of TBSA, fluid resuscitation should be initiated as soon as IV/IO access is established. Initiate resuscitation with (order of preference) Lactated Ringer’s, Plasma-Lyte A/Normosol-R, or normal saline.
- Analgesia in accordance with the K9TCCC Guidelines in Section 12 may be administered to treat burn pain
- Prehospital antibiotic therapy is not indicated solely for burns, but antibiotics should be given per the K9TCCC Guidelines in Section 13 if indicated to prevent infection in penetrating wounds.
- All K9TCCC interventions can be performed on or through burned skin in a casualty.
- Burn patients are particularly susceptible to hypothermia. Extra emphasis should be placed on barrier heat loss prevention methods.
17. Splint Fractures and Recheck Pulses
- IMPORTANT: Handle an injured K9 with a fracture with extreme care and proper restraint and muzzling. Consider sedation and analgesia before manipulating the fractured site (see section 12).
- Splints can be applied below the knee or elbow to stabilize the joint above and below the fracture. Ensure sufficient padding is in place along pressure points when applying these splints to minimize the risk of further injuries
Figure 35. Apply 1" medical adhesive tape stirrups to the inside and outside (or top and bottom) of the foot.
The ends of the tape should extend 4-6 inches beyond the toes.
Place a tongue depressor between the sticky sides of the tape so that the tape doesn't stick to other bandaging material.

Figure 36. Wrap cast padding around the limb, starting at the toes and past the joint above the fracture

Figure 37. Mold universal splint to outside portion of the fractured limb.
Center the splint over the fracture site.
Long aspect of the splint oriented along long aspect of the limb.
Mold the splint as best as possible to increase stability.

Figure 38. Wrap gauze bandage tape around splint
Wrap from the toes, up the limb. Wrap snugly but not so tight as to cut off circulation.

Figure 39. Remove the tape stirrups from the tongue depressor, twist 1/2 turn, and stick to the bandage material on each side of the paw

Figure 40. Wrap Elastikon /Coban tape around the gauze bandage
Wrap from the toes, up the limb. Wrap snugly but not so tight as to cut off circulation.

Figure 41. Write the date and time of the bandage on a piece of white medical adhesive tape

18. Cardiopulmonary Resuscitation (CPR)
- Resuscitation on the battlefield for victims of blast or penetrating trauma who have no pulse, no ventilations, and no other signs of life will not be successful and should not be attempted.
- However, K9 casualties with torso trauma or polytrauma who have no pulse or respirations during TFC should have bilateral needle decompression performed to ensure they do not have a tension pneumothorax prior to discontinuation of care. The procedure is the same as described in section 7a above.
The fillable electronic K9 Treatment and Resuscitation Record and instructions are available at:
https://jts.health.mil/assets/docs/forms/DD_3074_Canine_Treatment_and_Resuscitation_Record.pdf


19. Communication
- Communicate consistently with the K9 handler or assigned escort. Explain care provided and request support required for K9 management and positioning. Handler and K9 should travel together whenever feasible to facilitate handling and comfort of the K9.
- Communicate with tactical leadership as soon as possible and throughout K9 casualty treatment as needed. Provide leadership with K9 casualty status and evacuation requirements to assist with coordination of evacuation assets. Include K9 handler or escort in evacuation planning for casualty management (i.e. non-medical attendant).
- Communicate with the established evacuation system (the Patient Evacuation Coordination Cell) to arrange TACEVAC. Communicate with medical providers on the evacuation asset if possible and relay mechanism of injury, injuries sustained, identified signs/symptoms, and treatments rendered. Ensure receiving medical providers are aware of the need to have K9 Handler or assigned escort accompany the casualty for management.
20. Documentation of Care
- Document clinical assessments, treatments rendered, and changes in the K9 casualty’s status on a K9TCCC card (DD Form 3073). Forward this information with the casualty to the next level of care. Request general information from Handler or assigned escort.
The fillable electronic K9TCCC care and instructions are available at:
https://jts.health.mil/assets/docs/forms/DD_3073_Canine_Tactical_Combat_Casualty_Care_Card.pdf
https://jts.health.mil/assets/docs/forms/DD_3073_Instructions_Canine_Trauma_Combat_Casualty_Card.pdf

General Instructions for the K9TCCC Card (DD Form 3073)
PURPOSE: The K9TCCC Card is to provide standardized and consistent documentation of prehospital care by the Military Departments (MILDEPs) for Department of Defense (DoD) Working Dogs for trauma and disease non-battle injuries (DNBI).
The K9TCCC Card is filled out by the handler or provider who attends to the K9’s injuries or DNBI. After medical treatment and resuscitation care is provided, the K9TCCC Card must stay with the K9 when handed off to the next treatment facility to provide information regarding continuity of care.
At conclusion of care, the K9TCCC Card must be uploaded to the K9’s electronic Veterinary Health Record (eVHR). The K9TCCC Card will also be emailed to dha.mwdtraumaregistry@health.mil for inclusion into the DoD Military Working Dog Trauma Registry.
INSTRUCTIONS FOR COMPLETING DD FORM 3073 (FRONT OF CARD):
EVACUATION CATEGORY (Mark as appropriate.)
- URGENT – K9 who should be evacuated as soon as possible and within 1 hour to save life, limb, or eyesight and to prevent complications of serious illness and to avoid permanent disability.
- PRIORITY – K9 who should be moved within 4 hours, or their condition will deteriorate to such a degree that they will become an urgent precedence or whose requirements for special treatment are not available locally or who will suffer unnecessary pain or disability.
- ROUTINE – K9 whose condition requires evacuation but whose condition is not expected to deteriorate significantly and who will require evacuation in the next 24 hours.
EVACUATION TYPE (Mark as appropriate.)
K9 IDENTIFICATION
- UNIT – Record the unit to which the DoW WD is assigned.
- K9 NAME – Self-explanatory.
- TATTOO – Self-explanatory. Typically located on the inside of the ear
- DATE – DD-MM-YY
- TIME – Record all time local 24-hour military format as hh:mm.
- SEX – Mark as appropriate.
- MECHANISM OF INJURY – Mark as appropriate–use other for Disease Non-Battle Injuries or if unknown-describe.
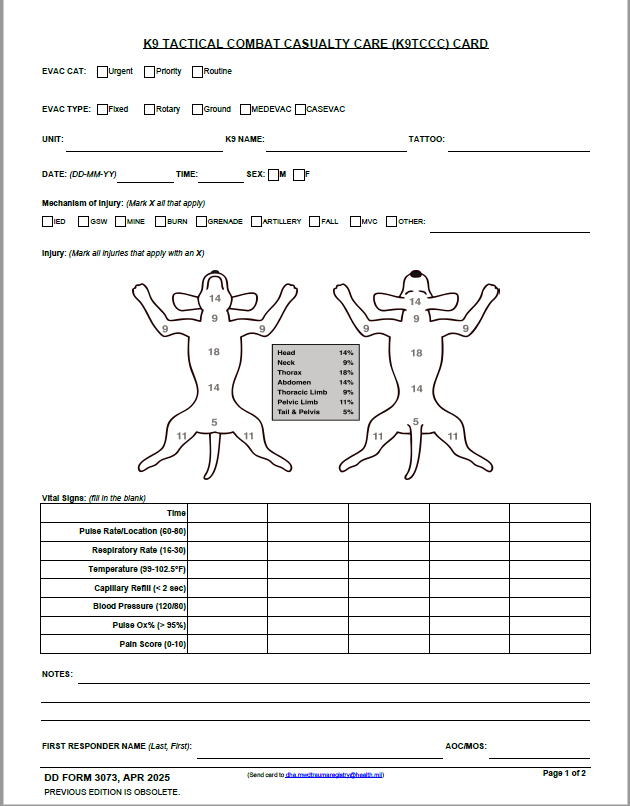
INJURY (Mark the diagram where the trauma/injury or disease is located–if there is more than one injury, identify each with the mechanism of injury.)
- The percentage numbers are provided as a reference when estimating K9 casualty burn injuries. If burn injuries have been sustained, the estimated percent burned should be annotated in the notes.
VITAL SIGNS (Input vital signs at least hourly.)
Pain Score:
0: Pain free
1 – 2: Mild pain; subtle weight shifting or subtle delay in lying down; enjoys being touched and petted.
3 – 4: Moderate pain; intermittent panting; delayed or slowed movement, subdued, weight shifting, likes to be touched except near or on injury, mild body tension.
5 – 6: Moderate to severe pain; looks uncomfortable when resting, anxious; pulls away when injury touched, moderate body tension.
7 – 8: Severe pain; unsettled, crying, biting or chewing at wound; difficulty maintaining comfortable position; increased respiratory rate, guards painful area, significant body tension when injury touched.
9 –10: Worst pain possible; panting; constantly groaning or screaming when unattended, may be aggressive to palpation, cries at non-painful palpation, severe body tension.
NOTES (Include any additional information such as location/country, euthanized/KIA, treatment regiments that were used to the treat the patient, etc.)
FIRST RESPONDER NAME (Self-explanatory)
AOC/MOS (Self-explanatory)
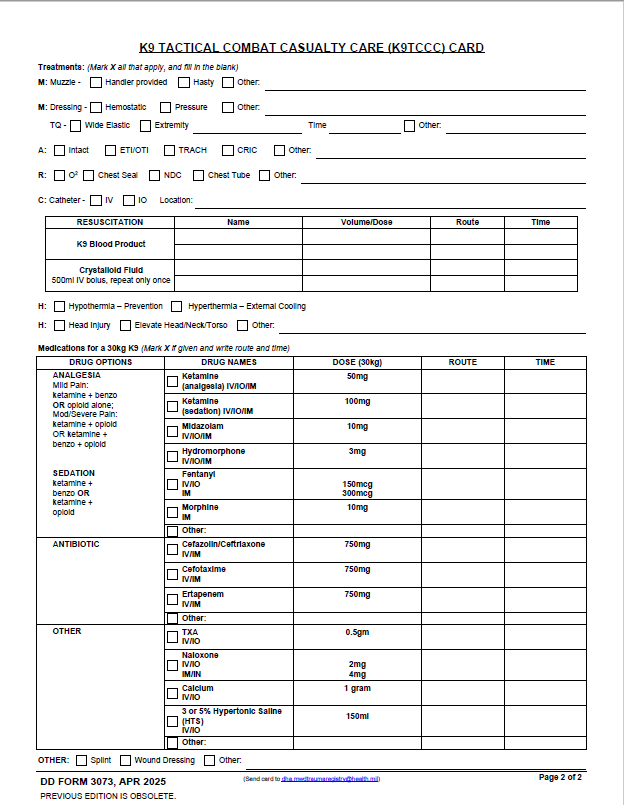
INSTRUCTIONS FOR COMPLETING DD FORM 3073 (BACK OF CARD):
TREATMENTS (Mark as appropriate and annotate location where appropriate.)
M (Muzzle): Mark as appropriate.
M (Massive Hemorrhage): Mark as appropriate.
A (Airway Control): Mark as appropriate.
R (Respiratory Support): Mark as appropriate.
C (Circulation):
CATHETHER (Mark as appropriate.)
FLUIDS (Fill out as appropriate and complete as possible.)
H (Hypo/hyperthermia): Self-explanatory.
H (Head Injury): Self-explanatory.
MEDICATIONS (Mark the medication given and write the route and time.)
OTHER (Self-explanatory.)
For additional information regarding the use of the DD Form 3073, please refer to the Defense Health Agency – Procedural Instruction 6040.47-V5.

READ FULL PDF
21. Prepare Casualty for Evacuation
- Complete and secure the K9TCCC Card (DD 3073) to the K9 casualty.
- K9 should remain muzzled if no concern for airway obstruction or respiratory distress. Secure muzzle to the K9 casualty for transport if it cannot be placed due to airway injury.
- Secure all loose ends of bandages and wraps.
- Provide instructions to K9 handler/escort as needed.
- Stage K9 casualties for evacuation in accordance with unit standing operating procedures.
- Maintain security at the evacuation point in accordance with unit standard operating procedures.
Principles of Tactical Evacuation Care (TACEVAC)
Principles of Tactical Evacuation Care (TACEVAC)
* The term “Tactical Evacuation” includes both Casualty Evacuation (CASEVAC) and Medical Evacuation (MEDEVAC) as defined in Joint Publication 4-02.
Basic Management Plan for Tactical Evacuation Care
Transition of Care
- Tactical force personnel should establish evacuation point security and stage K9 casualties for evacuation. K9 casualties must be accompanied by the handler or an assigned escort. The handler/escort should be designated to assist with K9 restraint and positioning.
- Tactical force personnel, the medic or the handler should communicate patient information and status to TACEVAC personnel as clearly as possible. The minimum information communicated should include stable or unstable, injuries identified, and treatments rendered.
- TACEVAC personnel should stage K9 casualties (with handler/escort) on evacuation platforms as required.
- Secure K9 casualties in the evacuation platform in accordance with unit policies, platform configurations and safety requirements.
- TACEVAC medical personnel should reassess K9 casualties and re-evaluate all injuries and previous interventions.
Massive Hemorrhage (same as Tactical Field Care)
Airway Management (same as Tactical Field Care)
Respiration/Breathing
Administration of oxygen may be of benefit for the following types of K9 casualties:
- Low oxygen saturation by pulse oximetry (<90%)
- Injuries associated with impaired oxygenation
- Unconscious casualty
- K9 casualty with a head injury (maintain oxygen saturation >90%)
- K9 casualty in shock
- K9 casualty at altitude
- Known or suspected smoke inhalation
Circulation (same as Tactical Field Care)
Head Trauma
K9 casualties with head trauma should be monitored for:
- Decreases in level of consciousness
- Pupillary dilation
- SBP should be >90mmHg
- O2 saturation >90%
- Hypothermia
- End-tidal CO2 (If capnography is available, maintain between 35-40 mmHg)
- Penetrating head injury (if present, administer antibiotics)
Pupillary dilation accompanied by a decreased level of consciousness, and dramatic changes in posture may signify impending cerebral herniation; if these signs occur, take the following actions to decrease intracranial pressure:
- Administer 150ml of 3 or 5% hypertonic saline IV/IO bolus over 2-5 minutes.
- Elevate the K9 casualty’s head, neck, and torso in line 30 degrees.
- Intubated K9 casualties should be ventilated to achieve an end-tidal CO2 between 30-35mmHg.
- The highest oxygen concentration (FiO2) possible should be used for ventilation.
Hypothermia Prevention (same as Tactical Field Care)
Penetrating Eye Trauma (same as Tactical Field Care)
Monitoring (same as Tactical Field Care)
Analgesia (same as Tactical Field Care)
Antibiotics (same as Tactical Field Care)
Inspect and Dress Known Wounds (same as Tactical Field Care)
Check for Additional Wounds (same as Tactical Field Care)
Burns
Splint Fractures
Cardiopulmonary Resuscitation (CPR) in TACEVAC
- Casualties with torso trauma or polytrauma who have no pulse or respirations during TACEVAC should have bilateral needle decompression performed to ensure they do not have a tension pneumothorax. The procedure is the same as described in Section (7a) above.
- CPR may be attempted during this phase of care if the K9 casualty does not have obviously fatal wounds and will be arriving at a facility with a surgical capability within a short period of time. CPR should not be done at the expense of compromising the mission or denying lifesaving care to other casualties.
Communication
- Communicate with the K9 handler or assigned escort. Explain care and any further requests for restraint or positioning.
- Communicate with veterinary personnel or medical providers at the next level of care as feasible and relay mechanism of injury, injuries sustained, signs/symptoms, and treatments rendered to K9. Provide additional information as appropriate.
Documentation of Care (same as Tactical Field Care)
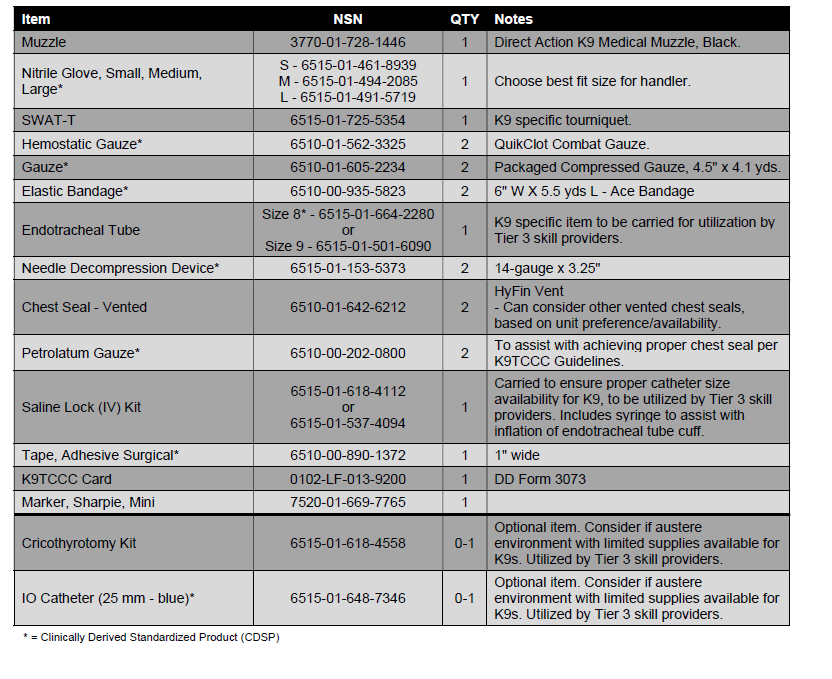
2023 K9TCCC Guidelines Annex - K9C4 K9 First Aid Kit
Below are the K9C4's recommendations for the K9 First Aid Kit, derived from the 2023 K9TCCC Guidelines.
These items are to be carried by the K9 handler (similar to an IFAK), to provide lifesaving point of injury K9 care. Training for this care is provided in the Tier 2 K9TCCC Course found on the Deployed Medicine website. Some K9 specific Tier 3 care level items are included to ensure availability in an operational environment.
It is the responsibility of the K9 unit to procure these items. They should be organized into a small, carried kit that is best fit to the unit's mission.
Most items are stocked in Theater Lead Agent for Medical materiel (TLAMM) assemblages and can be obtained through standard military supply channels. Items not included in assemblages can be purchased through suppliers by looking up the items NSN.
Familiarization of these items is provided in Module 2 "Medical Equipment" of the Tier 2 K9TCCC Course that can be found on the Deployed Medicine website.