The Use Of Dried Plasma In The Deployed Trauma System And Contingency Operations
Joint Trauma System
The Use Of Dried Plasma In The Deployed Trauma System And Contingency Operations
Damage control resuscitation is a bundle of care consisting of early transfusion with whole blood (WB) or balanced component therapy, early hemorrhage control, minimal use of crystalloid, administration of tranexamic acid (TXA), and rapid transport to forward surgical care.1-5 Data indicates that if (1) blood products are transfused within 36 minutes from wounding6 and (2) a casualty makes it to a surgical capability within 60 minutes, patient survival is improved (> 80% reduction in mortality risk).7-9 Early transfusion saves lives. However, whole blood or balanced component therapy transfusion is not always available in prehospital or logistically constrained environments. 10
While whole blood remains the preferred resuscitative fluid for bleeding patients; 11,12 in the absence of whole blood, a balanced component therapy ratio resuscitation (1:1:1) should be performed.13 Plasma is an integral part of a balanced or ‘hemostatic’ resuscitation.14,15 Dried plasma (DP), as opposed to liquid or fresh frozen plasma, has logistical advantages given that it is temperature stable and has a long shelf life, making it ideal for operational environments. Early administration of plasma has been demonstrated to decrease mortality.16,17 This guideline underscores that dried plasma is a complement to, not a replacement for, whole blood or balanced component resuscitation. Whole blood remains the preferred resuscitative fluid for severe hemorrhage, but dried plasma provides a critical contingency option when WB or liquid plasma are not readily available.18,19 Dried plasma has the potential to bridge the gap between injury and balanced resuscitation by restoring coagulation factors and volume support in the far-forward setting.20,21 Dried plasma is a universal product that can be administered to any patient regardless of blood group.
The Military Health System has begun fielding dried plasma to U.S. Military forces under two separate Emergency Use Authorizations (EUAs).
It is important to note that dried plasma is not a novel therapy. Its use represents the reintroduction of a once proven but long-absent resuscitative product, updated with modern safety standards and manufacturing methods to minimize transfusion transmitted infection and adverse reactions.22 This renewed development reflects the emphasis of early transfusion as well as operational demands of future combat casualty care within expeditionary environments where medical providers require flexible and reliable resuscitation strategies under conditions of constrained logistics.20
Dried plasma represents an important capability for austere and forward operational environments where conventional plasma is unavailable. Unlike liquid or fresh frozen plasma, dried plasma does not require cold chain support, is stored at room temperature for extended periods, and rapidly reconstitutes with sterile water at the point of care.
HISTORY & EVOLUTION OF DRIED PLASMA IN BATTLEFIELD MEDICINE
The use of dried plasma on the battlefield dates back to World War II. The U.S., Canada, and U.K. produced pooled freeze-dried plasma to treat combat casualties. These early preparations, while lifesaving, carried a high risk of transmitting hepatitis due to the pooling of plasma from multiple donors before the advent of modern viral testing. By the late 1950s, concerns over safety led the U.S. Military to discontinue its use of dried plasma, shifting instead to fresh frozen plasma (FFP) and later component therapy supported by an expanding cold chain infrastructure. 23-25
Freeze dried plasma (FDP) at one point became the preferred treatment for hemorrhage secondary to its ease of use compared to WB, however, it was a lesson learned in World War II that WB is necessary for hemorrhaging casualties and that FDP is only a bridge to whole blood, but one that could potentially be a successful Golden Hour extender.

In contrast, other nations continued to refine and employ dried plasma. The German military introduced a freeze-dried plasma product, which saw widespread use in World War II and was further developed for Bundeswehr use in later decades by the German Red Cross. The French military adopted dried plasma in the 1940s and has maintained its use into the present day, deploying it in both combat and humanitarian missions.26,27 Tens of thousands of units of French FDP have been administered safely, providing the most extensive modern clinical experience with this product type.
This historical record demonstrates that dried plasma is neither experimental nor untested. Rather, it has a long legacy of use on the battlefield, now being modernized for safety and integrated into contemporary trauma systems. By revisiting and updating its role in combat casualty care, dried plasma can once again fill a critical gap in forward resuscitation, particularly when cold chain logistics cannot support conventional plasma or WB delivery. Current dried plasma development complies with cGMP manufacturing, ensuring safety and traceability consistent with modern Food and Drug Administration (FDA) oversight. Modern processes such as solvent/detergent treatment, nanofiltration, and pathogen inactivation have been key to preventing the disease transmission concerns that halted its use in the United States after World War II.
Dried plasma is currently being fielded in the U.S. Military as a contingency product intended for forward deployed environments when WB or balanced component therapy is unavailable. It is not a replacement for whole blood or hemostatic resuscitation. Documentation of all dried plasma use is critical to inform future clinical recommendations and support a data-driven battlefield trauma system.
CONSIDERATIONS: USE OF DRIED PLASMA IN DEPLOYED ENVIRONMENTS
Currently, there are renewed clinical and operational needs that have driven NATO militaries, including Germany, Norway, and France, to prioritize dried plasma in their resuscitation strategies. The U.S. Department of War, Health and Human Services’ Biomedical Advanced Research and Development Authority, and academic centers have reinitiated research and development programs to bring freeze-dried and spray-dried plasma products to licensure under FDA oversight. Multiple investigational products are currently in preclinical or clinical evaluation. As these products are fielded to operational environments, documentation of use and outcomes will be required for the medical record and if the product is under an EUA by the FDA.
While several manufacturers are developing innovative freeze-dried (lyophilized) and sprayed-dried formulations of dried plasma, as of the date of publication for this CPG, the U.S. Military has fielded two dried plasma products under an EUA from the FDA; (1) Pathogen-Reduced Leukocyte-Depleted Freeze Dried Plasma manufactured by the Centre de Transfusion Sanguine des Armees (further referred to as “French FDP or FLYP”) and (2) octaplasLG Powder manufactured by Octapharma USA. Both of these formulations utilize pooled plasma and a freeze-drying process to produce a shelf stable powder in a glass bottle for reconstitution with sterile water at the point of care. There are no comparative efficacy studies that have evaluated clinical outcomes from use of the different types of dried plasma in bleeding patients. As the military fields more than one type of dried plasma, it is imperative that clinical documentation occurs to better understand the resuscitative efficacy of these products.
Multiple planning considerations should be accounted for when fielding dried plasma to the unit level. Both available formulations are manufactured in a glass bottle with risk of breakage if not adequately protected during transportation and storage in tactical environments. Additionally, the volume of sterile water for reconstitution is unique for each manufacturing process and must be adhered to. There are unique attributes of rigid glass bottle storage that require a vented administration line to allow flow of the reconstituted plasma. It is not possible to utilize pressure bags, pressure infusers or “squeezing the bag” to increase flow rates during administration; therefore, anticipate potentially slower administration times. The manufacturers of both French FDP and octaplasLG Powder recommend using filtered administration lines (included in the packaging) given the theoretical risk of infusing residual particulate matter that were not fully reconstituted. While both products are shelf stable for two years when stored between 2-25 degrees Celsius (35.6°F-77°F), degradation of coagulation factors and proteins should be expected if prolonged and extreme temperature excursions occur in storage or tactical employment.
The FDA has placed requirements for U.S. Military utilization of dried plasma products under their respective EUAs, to include specific training, documentation and reporting mandates. Providers must familiarize themselves with the product specific requirements as outlined further in this CPG. Additional training resources can be found at deployedmedicine.com or the Joint Trauma System website at https://jts.health.mil/
INDICATIONS FOR DRIED PLASMA USE
- Casualties with life-threatening hemorrhage/coagulopathy where whole blood or balanced component resuscitation is not immediately available (potential Golden Hour Extender).
- As part of a balanced component therapy resuscitation as substitution for liquid or frozen plasma if they are not readily available.
- May be used aboard ships when other products are not available.
- Dried plasma may be used prior to determining the recipient’s blood group.
- It is most valuable in Role 1 and Role 2 environments, during prolonged casualty care, and during long-range or constrained evacuation scenarios where cold chain support is limited or absent.
- Long shelf life at room temperature.
- Light, compact, and portable; suitable for austere or constrained logistics environments.
- Rapid reconstitution at point of care.
- Demonstrated efficacy in correcting trauma-induced coagulopathy.
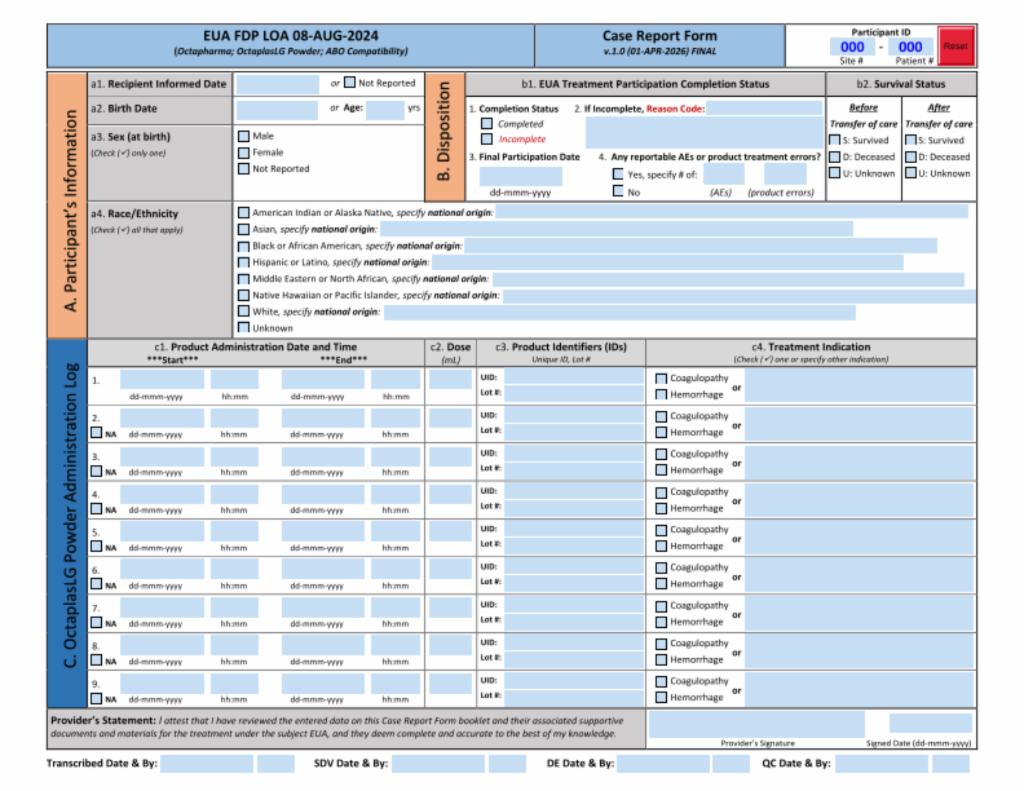
- For octaplasLG Powder, the documentation in the Case Report Form (CRF) must be filled out by providers and submitted.
- For French FDP, documentation of use will be provided to a site coordinator who will ensure completion of the CRF.
- The Serious Adverse Event (SAE) form is required in event of serious adverse events.
- Dried plasma provides coagulation factors for secondary hemostasis, but not red cell mass or platelets, and therefore must be integrated into a broader damage control resuscitation strategy that includes oxygen carrying capability and primary hemostasis.
- Factor V and VIII stability vary by product and may be lower compared to thawed plasma.
- General civilian use is not available, though an FDA Emergency Use Authorization has been granted for specific military applications.
- There are no comparative efficacy studies on the different types of dried plasma available.
- Dried plasma complements whole blood and component therapy by extending coagulation support until definitive transfusion is available.
- Dried plasma has the potential to bridge the time gap until whole blood or balanced component therapy can be administered prior to surgical hemorrhage control.
- It should be integrated into damage control resuscitation framework and should not be seen as a standalone capability, but as part of a bundle of battlefield resuscitation to include ASBP-supplied whole blood, balanced component therapy, walking blood banks, TXA, early hemorrhage control and prompt evacuation to forward surgical care.
DRIED PLASMA IMPLEMENTATION FOR EACH ROLE OF CARE
Tactical Combat Casualty Care (TCCC) Guidelines were developed to address care delivered in a prehospital environment prior to surgical capability where unique clinical and operational constraints differ from other battlefield roles of care. The TCCC Guidelines recognize tactical requirements and logistical constraints to include a limited number of medical responders, ongoing operations, constraints on cube/weight for medical equipment, and challenges with ensuring cold-chain storage for blood products.
Accordingly, TCCC recommends the following resuscitation fluids of choice for casualties in hemorrhagic shock, listed from most to least preferred:
1. Cold stored low titer O whole blood
2. Pre-screened low titer O fresh whole blood
3. Plasma, red blood cells (RBCs) and platelets in a 1:1:1 ratio
4. Plasma and RBCs in a 1:1 ratio
5. Plasma or RBCs alone
Dried plasma can be used when:
1. First line FDA compliant cold-stored low titer O whole blood is not available
2. Collection or transfusion of prescreened low titer O whole blood from a walking blood bank is delayed AND time-critical resuscitation warrants prompt volume resuscitation to stabilize a patient until fresh whole blood is available. Examples may include:
- Delayed donor response time following walking blood bank activation due to physical distance or enemy threat
3. Used as a liquid or fresh frozen plasma substitute in 1:1 resuscitation with RBCs, when conventional plasma products are not readily available
4. Neither whole blood nor traditional plasma components are readily available, to provide hemostatic support until able to perform a balanced resuscitation
ROLE 2 & ROLE 3: FORWARD SURGICAL CARE
At both Role 2 and Role 3 MTFs, dried plasma can be used as a critical adjunct to resuscitation strategies if whole blood is not immediately available. Dried plasma can also be treated as a regular plasma product within the damage control resuscitation framework. The use of dried plasma must be documented to include type of dried plasma product and the time of transfusion.
Dried plasma can be used when:
1. First line FDA approved cold-stored low titer O whole blood is not available
2. Collection or administration of second and/or third line products (fresh frozen or liquid plasma) is delayed AND time-critical resuscitation warrants prompt resuscitation to stabilize a patient until other products are available. Examples may include:
- Fresh frozen plasma has not been thawed and ready for transfusion.
- Delayed donor response time following walking blood bank activation due to physical distance or enemy threat.
- Time to fill out prescreening donor questionnaire impacts resuscitation (if donor pool has not been prescreened).
- Required time for rapid lab or point of care testing of previously unscreened donors.
- Required time for lab testing of previously unscreened donors at a lab capable facility.
3. Dried plasma can be used as an FFP or liquid plasma substitute in 1:1 resuscitation with RBCs.
Other considerations: Plasma has shown efficacy in both burn resuscitation and severe Traumatic Brain Injury (TBI). Many burn centers use plasma instead of crystalloid to resuscitate burn patients. For TBI, there is strong preclinical evidence that plasma decreases the size of hemorrhagic injury. The 2026 TCCC Guidelines adopted plasma use for TBI.
Dried plasma can be used in place of liquid plasma or FFP for both burn and TBI resuscitation. All uses must be documented; this cannot be overstated. Documentation of combat casualty care is how the battlefield trauma system evolves and care is improved.
Ensure dried plasma utilization (transfused or destroyed) is documented and EUA/SAE forms from prior roles of care are scanned into the Theater Medical Data Store/Theater Blood Mobile or appropriate operational blood IT system.
OCTAPLASLG POWDER PRODUCT ADMINISTRATION
The EUA for octaplasLG Powder allows use by “U.S. Military forces for the treatment of hemorrhage or coagulopathy during an emergency involving agents of military combat (e.g., firearms, projectiles, and explosive devices) when plasma is not available for use or when the use of plasma is not practical.”

Health care professionals or other authorized providers need to familiarize themselves with the fact sheet for providers (Appendix C) and with the following steps for product administration:
- Always use aseptic technique when connecting the transfusion set with the vented spike adaptor and the vial.
- Remove the blister from the transfusion set and the blister from the vented spike adaptor.
- Remove the protective cap from the spike of the transfusion set. Slide the vented spike adaptor onto the spike of the transfusion set. Then remove the protective cap from the spike of the adaptor.
- Connect the transfusion set with the adaptor to the powder bottle (octaplasLG Powder) by perforating the rubber stopper centrally with the spike of the adaptor.
- Ensure the spike is fully inserted into the vial so that liquid can flow through the tubing.
- Gently squeeze the drip chamber of the transfusion set to fill it partially with liquid.
- Transfuse the product according to your established clinical protocols. Patients’ vital signs should be closely monitored throughout the infusion as conditions permit.
- Repeat administration as medically necessary.
FRENCH FDP (FRENCH LYOPHILIZED PLASMA – FLYP) PRODUCT ADMINISTRATION
The EUA for French FDP (French Lyophilized Plasma - FLYP) allows use by “U.S. Military forces for the treatment of hemorrhage or coagulopathy during an emergency involving agents of military combat (e.g., firearms, projectiles, and explosive devices) when plasma is not available for use or when the use of plasma is not practical.”

Health care professionals or other authorized providers need to familiarize themselves with the fact sheet for providers (Appendix G) and with the following steps for product administration:
- Bring the two flasks (powder and solvent) to room temperature (+20°C to +25°C) (68°F- 77°F) if necessary.
- Remove the protective capsules from the two flasks.
- Disinfect the surface of each lid.
- Pierce the lid of the flask containing the water first with one of the bevels of the transfer set. Be sure that you spike the water first. If you accidentally spike the powder first, you will lose the vacuum and then be unable to transfer the water to the bottle of powder using the transfer set.
- Use the other bevel to pierce the lid of the flask containing the powder.
- Pour the entire contents of the water flask into the flask containing the powder via the transfer set.
- Gently agitate the flask making horizontal rotations without generating a foam (do not shake) to homogenize the mixture.
- Wait 3 to 5 minutes for the product to dissolve entirely before injecting.
- Before infusion, check that the glass flask is intact. Do not use the contents of a damaged flask under any circumstances.
- Obtain a set of pre-infusion vital signs if tactical conditions permit.
- Prior to infusion, you must open the vent on the sterile tubing set. Using the intravenous infusion set provided, immediately administer the entire preparation intravenously.
- Obtain a set of post-infusion vital signs if tactical conditions permit.
- Closely monitor the patient for signs of an adverse reaction (e.g., fever, rash, hives, difficulty breathing, flank pain, darkening urine) and for adequacy of resuscitation (return of radial pulse or improvement in systolic blood pressure to approximately 90 mm Hg, improvement in mental status, improved hemorrhage control).
PERFORMANCE IMPROVEMENT (PI) MONITORING
All trauma patients who receive Dried Plasma transfusion(s) as part of a resuscitation strategy, whether in lieu of or in conjunction with whole blood and/or balanced component blood products.
- Dried plasma will NOT be transfused when whole blood or balanced component therapies are readily available.
- Indication for transfusion of dried plasma will be clearly documented.
- The Dried Plasma Case Report Form will be completely filled out for each patient receiving dried plasma.
- Reconstitution of dried plasma products will be done only with sterile water, as reconstitution effects using products other than sterile water have not been tested.
- Pre- and post-transfusion vital signs will be clearly documented for each transfusion of dried plasma.
- All instances of adverse reaction will be documented on the Severe Adverse Event Form.
PERFORMANCE / ADHERENCE METRICS
- Instances of dried plasma transfusion in which the Dried Plasma Case Report Form was entirely completed and submitted.
- Dried plasma transfusion in accordance with specified indications and clear documentation of indication.
- Dried plasma product reconstituted with sterile water.
- Documentation of pre- and post-transfusion vital signs.
- Severe Adverse Event form was completed to document any adverse reaction or event.
- Blood transfusion databases: Theater Medical Data Store (TMDS) or Theater Blood Mobile
- DoD Trauma Registry
- Patient Record
- EUA forms
The above constitutes the minimum criteria for PI monitoring of this CPG. System reporting will be performed annually; additional PI monitoring and system reporting may be performed as needed. The system review and data analysis will be performed by the Joint Trauma System (JTS) Chief and the JTS PI team.
It is the trauma team leader’s responsibility to ensure familiarity, appropriate compliance, and PI monitoring at the local level with this CPG.
DOTMLPF-p

REFERENCES
- Thompson P, Strandenes G. The history of fluid resuscitation for bleeding. In: Spinella PC, ed. Damage control resuscitation: identification and treatment of life-threatening hemorrhage. Cham: Springer International Publishing, New York, New York; 2020:3–29.
- Beekley AC. Damage control resuscitation: a sensible approach to the exsanguinating surgical patient. Crit Care Med. 2008;36(7 suppl):S267–S274.
- Hess JR, Holcomb JB, Hoyt DB. Damage control resuscitation: the need for specific blood products to treat the coagulopathy of trauma. Transfusion. 2006;46:685–686.
- Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62:307–310.
- Nessen SC, Eastridge BJ, Cronk D, et al. Fresh whole blood use by forward surgical teams in Afghanistan is associated with improved survival compared to component therapy without platelets. Transfusion. 2013;53(Suppl 1):107S–113S.
- Cap AP, Pidcoke HF, Spinella P, et al. Damage control resuscitation. Mil Med. 2018 Sep 1;183(suppl_2):36-43.
- Shackelford SA, Del Junco DJ, Powell-Dunford N, et al. Association of prehospital blood product transfusion during medical evacuation of combat casualties in Afghanistan with acute and 30-day survival. JAMA. 2017 Oct 24;318(16):1581-1591.
- Shackelford SA, Del Junco DJ, Mazuchowski EL, et al. The golden hour of casualty care: rapid handoff to surgical team is associated with improved survival in war-injured US Service Members. Ann Surg. 2024 Jan 1;279(1):1-10.
- Kotwal RS, Scott LLF, Janak JC, et al. The effect of prehospital transport time, injury severity, and blood transfusion on survival of US military casualties in Iraq. J Trauma Acute Care Surg. 2018 Jul;85(1S Suppl 2):S112-S121.
- Fisher AD, Miles EA, Broussard MA, et al. Low titer group O whole blood resuscitation: military experience from the point of injury. J Trauma Acute Care Surg. 2020;89:834–841.
- Cap A, Beckett A, Benov A, et al. Whole Blood Transfusion, Military Medicine, Volume 183, Issue suppl_2, September-October 2018, Pages 44–51,
- Whole Blood Transfusion Clinical Practice Guideline, 15 May 2018. https://jts.health.mil/index.cfm/CPGs/cpgs
- Borgman MA, Spinella PC, Perkins JG, et al. The ratio of blood products transfused affects mortality in patients receiving massive transfusions at a combat support hospital. J Trauma. 2007;63:805–813.
- Giangrande PL, The history of blood transfusion. Br J Haematology. 2000;100:758–767.
- Beal RW. The rational use of blood. Aust N Z J Surg. 1976;46:309–313.
- Sperry JL, Guyette FX, Brown JB, et al. Prehospital plasma during air medical transport in trauma patients at risk for hemorrhagic shock. N Engl J Med. 2018 Jul 26;379(4):315-326.)
- Lewis RE, Muluk SL, Reitz KM, et al. Prehospital plasma is associated with survival principally in patients transferred from the scene of injury: A secondary analysis of the PAMPer trial. Surgery. 2022 Oct;172(4):1278-1284
- Sperry JL, Cotton BA, Luther JF, et al, Whole blood resuscitation and association with survival in injured patients with an elevated probability of mortality. J Am Coll Surg. 2023 Aug 1;237(2):206-219.
- Dorken-Gallastegi A, Spinella PC, Neal MD, et al. Whole blood and blood component resuscitation in trauma: interaction and association with mortality. Ann Surg. 2024 Dec 1;280(6):1014-1020.
- Gurney JM, Cap A, Holcomb JB, et al. The thin red line: Blood planning factors and the enduring need for a robust military blood system to support combat operations. Journal of Trauma and Acute Care Surgery 97(2S):p S31-S36, August 2024.
- Kalkwarf KJ, Cotton BA. Resuscitation for hypovolemic shock. Surg Clin North Am. 2017;97(6):1307–1321
- Association for the Advancement of Blood and Biotherapies. Transfusion medicine history. https://www.aabb.org/news-resources/resources/transfusion-medicine/highlights-of-transfusion-medicine-history. Accessed May 22, 2026.
- Hess JR, Thomas MJ. Blood use in war and disaster: lessons from the past century. Transfusion. 2003;43:1622–1633.
- Oberman HA. The indications for transfusion of freshly drawn blood. JAMA. 1967;199:93–97.
- Gonzalez EA, Moore FA, Holcomb JB, et al. Fresh frozen plasma should be given earlier to patients requiring massive transfusion. J Trauma. 2007;62:112–119.
- Pidcoke HF, Aden JK, Mora AG, et al. Ten-year analysis of transfusion in Operation Iraqi Freedom and Operation Enduring Freedom: increased plasma and platelet use correlates with improved survival. J Trauma Acute Care Surg. 2012 Dec;73(6 Suppl 5):S445-52.
- Spinella PC, Perkins JG, Grathwohl KW, et al. Warm fresh whole blood is independently associated with improved survival for patients with combat-related traumatic injuries. J Trauma. 2009;66(4 Suppl):S69–S76.
APPENDIX B: OCTAPLASLG POWDER FDA AUTHORIZATION LETTER FOR EMERGENCY USE AUTHORIZATION


APPENDIX F: FRENCH FDP (FRENCH LYOPHILIZED PLASMA – FLYP) FDA AUTHORIZATION LETTER FOR EMERGENCY USE AUTHORIZATION

APPENDIX I: FDA MED WATCH FORM 3500 (USED FOR BOTH OCTAPLASLG AND FRENCH FDP (FRENCH LYOPHILIZED PLASM A – FLYP)
Note: FDA Med Watch Form 3500 is used for both octaplasLG and French FDP (French Lyophilized plasma -FLYP)
APPENDIX J: MEDICAL MATERIEL CLASS VIII LIST
This itemized checklist supports implementation of the Use of Dried Plasma in the Deployed Trauma System and Contingency Operations CPG. These components represent the minimum materiel necessary to safely reconstitute, administer, and monitor dried plasma in accordance with the JTS CPG and the octaplasLG Powder EUA Fact Sheet.
octaplasLG Powder vial (A or AB plasma)
- Sterile water for Injection bag (190 mL)
- Manufacturer-provided transfer set
- Manufacturer-provided vented spike adaptor
- Manufacturer-provided transfusion set with 170–200 μm filter
French FDP/FLYP Powder vial
- Sterile water for Injection (200mL or 250mL)
- Manufacturer-provided transfer set
- Manufacturer-provided tubing set (toggle, in-line 200 μm filter, a vent, and needle for product administration)
- Alcohol prep pads (minimum 2 per unit)
- Sterile gloves
- Clean field or sterile drape
- Waste disposal bag/container environmental requirements
- Timer/watch for reconstitution monitoring
- Product should dissolve within approximately 15 minutes
- Discard if not fully dissolved within 30 minutes
- IV catheters 18 gauge, 16-gauge, 14-gauge
- IV extension tubing
- Saline flushes
- Transparent dressing
- IV securement tape alternative access
- Intraosseous (IO) device and needles when IV access cannot be obtained
- Vented transfusion set with 170–200 μm filter
- Vented spike adaptor
- IV pole or suspension device (optional)
- Blood pressure cuff
- Stethoscope
- Pulse oximeter
- Thermometer
- Cardiac monitor (if available)
- Vital signs documentation sheet pre and post-infusion
The EUA specifically highlights risks of transfusion reactions, anaphylaxis, TRALI, hypervolemia, and citrate toxicity.
Emergency Medications:
- Epinephrine 1 mg/mL (1:1000)
- Diphenhydramine
- Methylprednisolone or Hydrocortisone
- Calcium gluconate or calcium chloride
- For citrate-induced hypocalcemia airway and oxygen support
- Oxygen source
- Nasal cannula
- Non-rebreather mask
- Bag-valve-mask (BVM)
- Suction equipment
- DD Form 1380 TCCC Card
- Blood product administration record
- Serious Adverse Event Form (if needed)
- Patient monitoring/vital signs worksheet product tracking
- FDA Med Watch Form 3500
“One-Unit Dried Plasma Administration Kit” For an operational Role 1, prolonged casualty care, or far-forward team: The items that are unique and essential to octaplasLG powder administration are:
- octaplasLG powder vial
- Sterile water for injection (190 mL)
- Transfer set
- Vented spike adaptor
- Transfusion set with 170–200 μm filter
- Alcohol prep pads
- Large-bore IV/IO access
- Basic patient monitoring equipment
- Emergency medications for transfusion reactions
For additional information including National Stock Number (NSN), please contact dha.ncr.med-log.list.lpr-cps@health.mil
DISCLAIMER: This is not an exhaustive list. These are items identified to be important for the care of combat casualties.
APPENDIX K: TELEMEDICINE / TELECONSULTATION

APPENDIX L: INFORMATION REGARDING OFF-LABEL USES IN CPGS PURPOSE
The purpose of this Appendix is to ensure an understanding of DoD policy and practice regarding inclusion in CPGs of “off-label” uses of U.S. Food and Drug Administration (FDA)–approved products. This applies to off-label uses with patients who are armed forces members.
Unapproved (i.e. “off-label”) uses of FDA-approved products are extremely common in American medicine and are usually not subject to any special regulations. However, under Federal law, in some circumstances, unapproved uses of approved drugs are subject to FDA regulations governing “investigational new drugs.” These circumstances include such uses as part of clinical trials, and in the military context, command required, unapproved uses. Some command requested unapproved uses may also be subject to special regulations.
Additional Information Regarding Off-Label Uses in CPGs
The inclusion in CPGs of off-label uses is not a clinical trial, nor is it a command request or requirement. Further, it does not imply that the Military Health System requires that use by DoD health care practitioners or considers it to be the “standard of care.” Rather, the inclusion in CPGs of off-label uses is to inform the clinical judgment of the responsible health care practitioner by providing information regarding potential risks and benefits of treatment alternatives. The decision is for the clinical judgment of the responsible health care practitioner within the practitioner-patient relationship.
Consistent with this purpose, CPG discussions of off-label uses specifically state that they are uses not approved by the FDA. Further, such discussions are balanced in the presentation of appropriate clinical study data, including any such data that suggest caution in the use of the product and specifically including any FDA-issued warnings.
With respect to such off-label uses, DoD procedure is to maintain a regular system of quality assurance monitoring of outcomes and known potential adverse events. For this reason, the importance of accurate clinical records is underscored.
Good clinical practice includes the provision of appropriate information to patients. Each CPG discussing an unusual off-label use will address the issue of information to patients. When practicable, consideration will be given to including in an appendix an appropriate information sheet for distribution to patients, whether before or after use of the product. Information to patients should address in plain language: a) that the use is not approved by the FDA; b) the reasons why a DoD health care practitioner would decide to use the product for this purpose; and c) the potential risks associated with such use.
DOWNLOAD CPG IN PDF

READ FULL PDF