Interfacility Transport of Patients Between Medical Treatment Facilities
Joint Trauma System
Interfacility Transport of Patients Between Medical Treatment Facilities
- Document changed from a Clinical Practice Guideline (CPG) to CoERCCC Operational Guideline (OPG).
- Addressed ground transport considerations.
- Emphasis on communication between en route care commanders and echeloned medical directors prior to out-of-theater evacuation that is governed by U.S. Transportation Command (USTRANSCOM) and Theater-Specific Patient Movement Requirements Centers.
- Recommend protocol creation at the regional level by the medical director and modified at the local level on an as-needed basis.
INTRODUCTION
Reducing the time to required medical or surgical intervention prevents death in potentially survivable illnesses, injuries, and wounds. When evacuation times are extended, en route care (ERC) medical care capability must be adequately expanded to mitigate the delay. In January 2010, the Joint Force Health Protection Joint Patient Movement Report stated, “the current success of the medical community is colored by the valiant ability to overcome deficiencies through 'just-in-time workarounds.’ Many systemic shortfalls are resolved and become transparent to patient outcomes. However, future operations with peer or near-peer adversaries may not tolerate current deficiencies.” 1,2
This JTS Operational Guideline recommends the minimum requirements and capabilities for the movement of critical care patients between military medical treatment facilities (MTFs). ERC and patient movement play a critical role in the combat casualty care continuum. Short times to a ‘capability’ allow for life-saving intervention to be delivered shortly after illness or injury; this was the trauma system during previous U.S. Central Command (USCENTCOM) operations. Rapid transport through the care continuum was exploited during USCENTCOM operations to support the small medical footprint, forward surgical care, and rapid transport to a higher echelon of clinical care. This was made possible secondary to air superiority and numerous deployed Medical Evacuation (MEDEVAC) teams. In the future operating environment, ERC personnel may find themselves providing primary and emergent care with little possibility of timely patient movement. All providers should have familiarity with the risks, benefits, and alternatives to rapid movement of casualties and have a clear understanding and familiarity with all possible platforms in which they could be called upon to move patients in theater to the next role of care.
This guideline is specifically concerned with the administrative aspects of inter-facility transport of patients between the intra-theater roles of care. Please refer to the En Route Care guidelines (located on JTS website & Deployed Medicine) and to Aeromedical Evacuation (AE) guidelines for inter-theater transport. It is important to note that, in an immature theater of operations or in a larger-scale conflict, casualty numbers may exceed available resources. When this occurs, compliance with this guideline may be compromised.
Combatant Commanders need to ensure appropriate patient movement resources are a priority, especially for critical care transports between treatment facilities.
BACKGROUND
In recent conflicts, most combat deaths occurred before arrival at Role 3 facilities, underscoring the need for improved care.3 ERC is critical across the continuum, especially in Large Scale Combat Operations (LSCO), where higher casualty rates and evacuation constraints are expected.
Interfacility transport adds risk - movement often occurs in combat platforms with limited space, few providers, and challenging conditions—noise, vibration, cramped quarters, and weather—that compromise monitoring, dislodge equipment, and worsen injuries.4,5 Air transport adds further hazards, including reduced oxygen pressure and increased tissue swelling.6 Enemy activity and diplomatic restrictions can also impact routes, timing, and safety. Effective ERC teams anticipate these threats and develop strategies to mitigate them to the best of their abilities.
Patient transport itself is a medical intervention with inherent risks and benefits. In combat, evacuation is essential to deliver definitive treatment and clear the battlefield. Medical resource centralization reduces relocation needs, preserves capability, and lowers logistical burden. Still, each movement carries both direct risk to patients and the possibility of losing transport assets and crews to accidents or enemy action.
Patient Stabilization
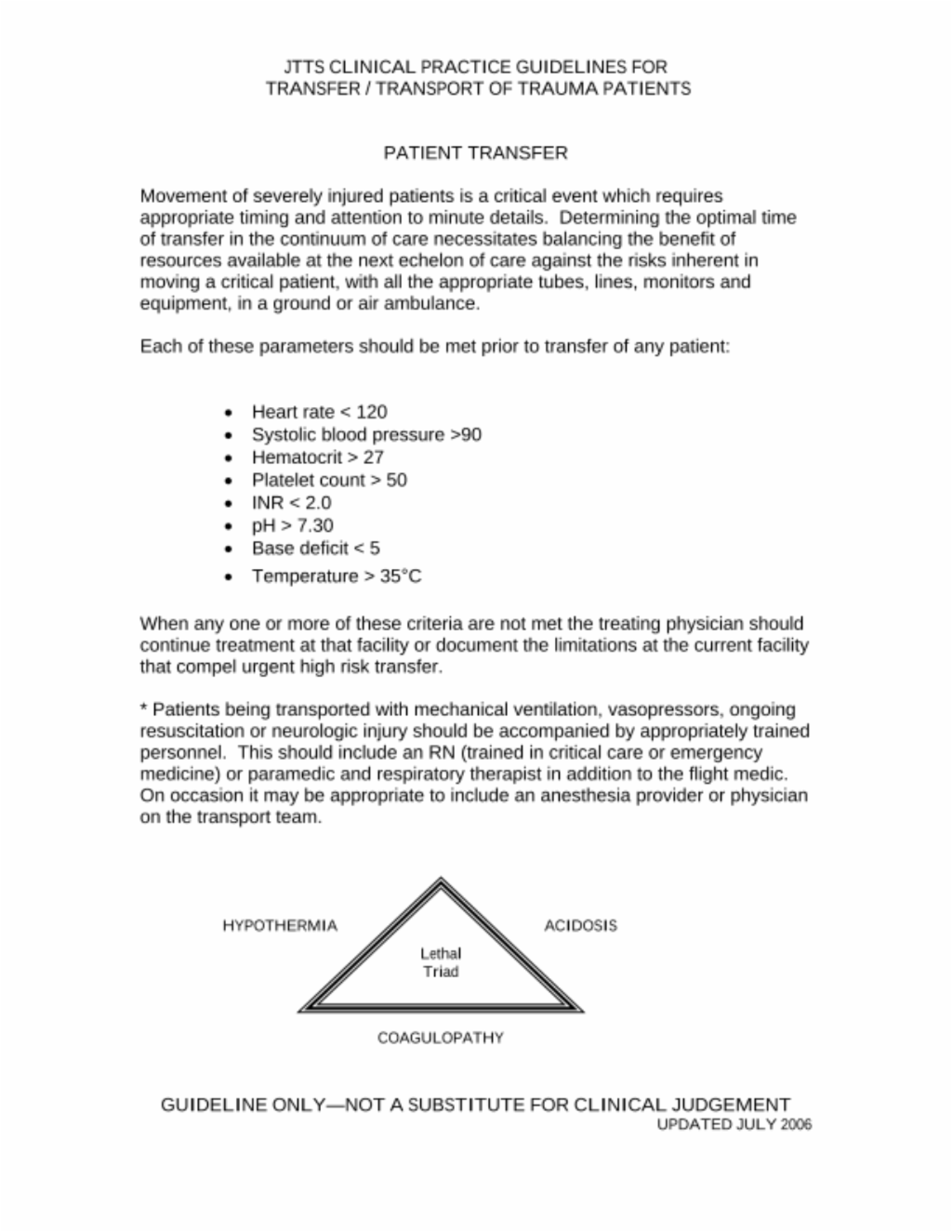
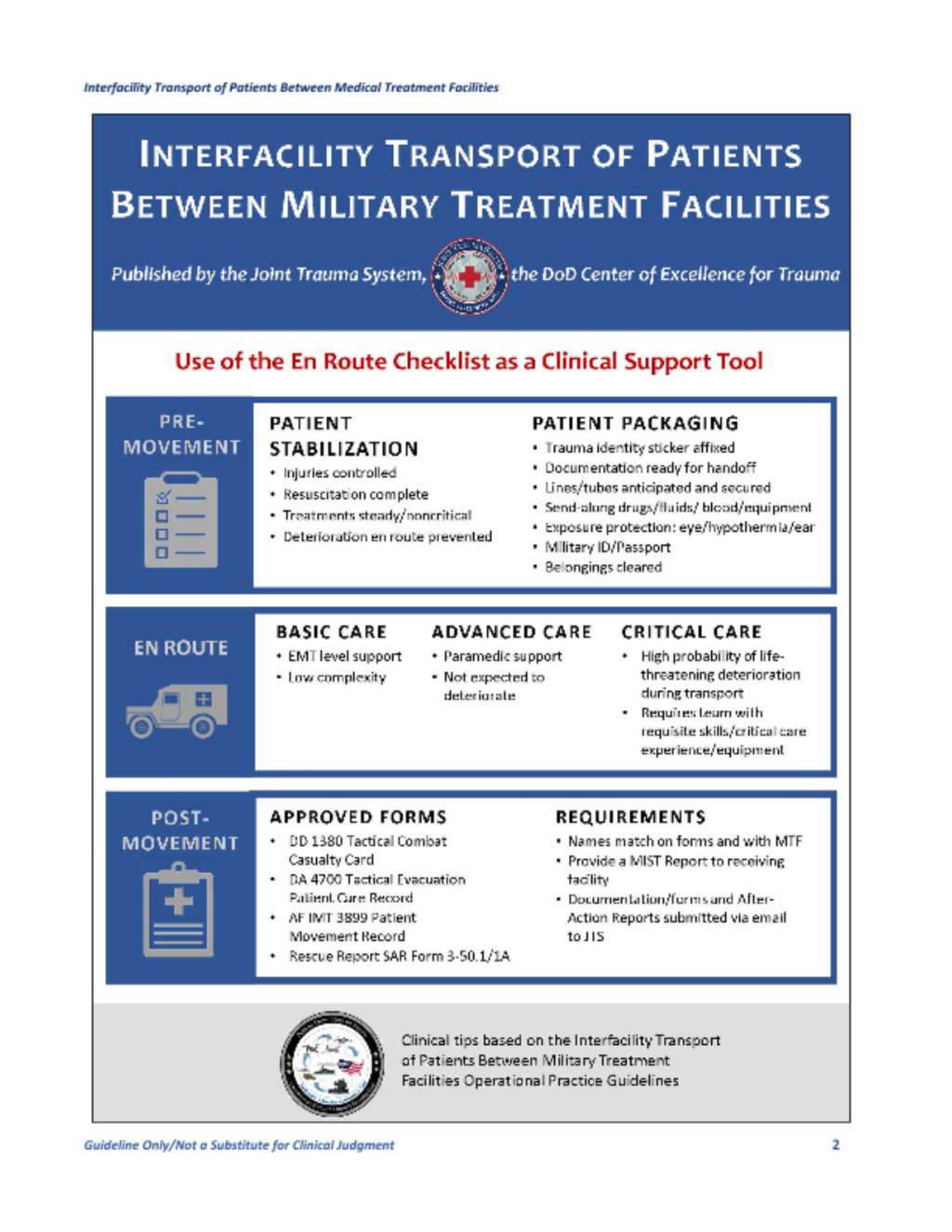
To minimize transport contribution to morbidity and mortality, optimal but not necessarily definitive patient stabilization before transport is critical and encompasses four connected elements:
- Injuries—actual and potential (e.g., spinal instability)—must be controlled. This usually happens at the earliest phase of tactical combat casualty care.
- Resuscitation must be optimized but may be ongoing. The best outcomes occur when a patient’s physiology is closest to normal before transport.7,8 Patient variables that best indicate adequate resuscitation for transport continue to be an area for continued basic and translational research.9,10,11,12 The parameters outlined in Table 1 serve as a general guide for adequate resuscitation goals. High-risk patients or critical care patients require intensivist-led en route critical care and collaboration between the ERC team’s physician and the local medical director. Furthermore, if the patient requires ongoing resuscitation and goals are not met before transport, there must be documentation of reasons for transport and a clear outline of risk mitigation steps. Other treatments besides resuscitative measures should be at steady-state, not requiring dynamic, complex, or life-preserving adjustments en route. Until technology progresses, the planned initiation of new interventions or the continuation of complex or capability unique interventions during transport are discouraged.
- Clinical deterioration requiring en route intervention must be anticipated and prevented with risk mitigation procedures prior to departure. Examples include placing lines or tubes, or decompressing compartment syndromes, as well as providing adequate analgesia for the increased pain of transport. This requires an understanding of the injury course as well as the transport environment.
- Preparation for transport must include more than just patient physiology. Packaging to ensure safety during the transitions of care is also essential. This includes the logistical and the indirect clinical aspects of preparing the patient for transfer from the treatment facility to the ERC team. Many of these steps can be managed by the non-physician members of the transferring team but must be verified by the ERC providers prior to departure. For a more detailed guide on how to package patients, see En Route Care Patient Packaging, 21 Aug 2024.
Resuscitation Goals
1. Heart Rate 50-120 /min
2. SBP >90 mm Hg, MAP >60 mm Hg - in the absence of traumatic brain injury
If elevated ICP or CPP, maintain target MAP between 80-110 mmHg
3. SpO2 >94%
4. Temp > 95ºF/35ºC
5. Urine Output > 50 mL/h
6. Hemoglobin > 7.0 g/dL
7. Platelets > 50k/mm³
8. INR < 2.0
9. Base Deficit < 6
10. Lactate < 2.5 mmol/L
11. EtCO2 35-45 mmHG
Expected ERC Capabilities
Medical capability is the quality or state of being able to provide the expected and required medical services and support to the patient. Within the system of ERC, and when capability is discussed in this document, it is the ready and available potential to provide the required critical care in a proficient and timely manner. It includes the physical and mental talent of the team, as well as the physical presence of all medical materials and equipment in the platform that are expected by theater policy. A capability does not exist if the personnel are not proficient or if they are missing medical supplies and equipment. The ERC team must be integrated effectively with the transport platform team. The ERC team should be integrated effectively with the transport platform team. Therefore, units must be conversant and compliant with the published theater standards, along with being physically and materially ready to execute the assigned mission. Within the operational theater, it is critical to ensure actual capability is effectively communicated between medical control, the transferring facility, the ERC team, and the receiving facility. The ERC organization has a moral, ethical, and legal obligation to ensure they can carry out their mission essential task list and mission essential care capability for the patient. If not, they must notify their commander, the medical director, and the medical dispatch center that they are unable to provide the expected and required care to our critically ill, injured, or wounded patients. Since MEDEVAC is a theater asset, the local unit commander cannot legitimately accept risk for the theater commander. Locally accepting risk of a reduced capability compromises care, contributes to excess morbidity and mortality, and is inconsistent with the effective and efficient use of medical dispatch centers. It is the center’s mission to select and assign the appropriate evacuation asset to the right mission.
Three levels of capability are recognized in this guideline: Basic, Advanced, and Critical Care. The ideal military ERC system will be a scalable and modular asset with appropriate resource allocation to provide a full range of patient care services, including advanced clinical capabilities.
Basic ERC should be initiated for a patient capable of being transported by ground ambulance that does not require critical care but needs a dedicated medical attendant with at least the knowledge and skills equivalent to an Emergency Medical Technician (EMT) as defined by the National EMS Scope of Practice Model. Adequate medical supplies to perform basic lifesaving interventions are necessary. Patients in this category have a low complexity of care requirement, which must be attended by a medically skilled provider, but are not expected to deteriorate during the period of the patient movement.
Advanced ERC should be initiated for a patient who does not require critical care but needs a dedicated medical attendant with at least the knowledge and skills equivalent to a paramedic as defined by the National Emergency Medical Services (EMS) Scope of Practice Model.14 Adequate medical supplies to perform lifesaving interventions, as well as ongoing resuscitation, are also necessary. Patients in this category have some complexity of care delivery that must be maintained by a medically skilled provider but are not expected to deteriorate during the period of the patient movement.
Critical Care Transport is required when “the patient has a critical illness or injury which acutely impairs one or more vital organ systems such that there is a high probability of imminent or life-threatening deterioration in the patient's condition during transport.” For success, en route critical care must be provided by a team of providers “with the requisite decision making skills of high complexity to assess, manipulate, and support vital organ system failure and/or to prevent further life threatening deterioration of the patient's condition during transport.”13 Ideally, this multidisciplinary team will be comprised of a physician or other independent practitioner with extensive critical care experience, an ERC-trained Critical Care or Emergency Nurse, and a Flight Paramedic. This team will have the requisite equipment to perform lifesaving interventions as required by the clinical scenario.
Sometimes, a completely packaged and fully stabilized patient is operationally unrealistic. Some injuries or illnesses cannot be stabilized due to capability limitations. Limited capability may be the driving indication for transport. These transfers are fraught with the risks of undesired outcomes during transport. Subsequently, the transferring provider should document the indications for transport before patient movement, continue the resuscitation, and ensure adequate (even higher) capability of the ERC. The gold standard for unstable patient transport is movement with critical care capability led by a physician who is qualified, experienced, and proficient at critical care transport.
Required ERC capability should be based on the current condition of the patient being transferred and their expected course during transport. This is determined by the transferring provider. If the requested level of ERC is not available, then a higher level of care should be provided. If this is not an option, then the transferring provider and the operational commander must carefully weigh the risks of patient transfer using a lower capability versus the risks of transport delay.
Commanders
Joint Publication 1 Joint Publication Vol 1, Joint Warfighting, 27 Aug 2023 states that, “…doctrine will be followed except when, in the judgment of the commander, exceptional circumstances dictate otherwise.” The Commanders have specific responsibilities under Title 10, United States Code, to organize, train, equip, prepare, and maintain their forces. For the purposes of this document, that responsibility is the ERC capability. Commanders are delegated authority to accomplish their assigned missions but cannot absolve themselves of responsibility for the attainment of these missions.
Commanders of dedicated MEDEVAC organizations shall not individually assume risk when they are not capable of providing the required intratheater ERC capability. Any risk assumption of reduced capability should be assumed by the theater commander, as MEDEVAC is a theater-level responsibility. It is the commander’s duty to notify higher command if they cannot execute their mission essential task list. Inherent to ERC within the mission essential task list is the capability to care for the patient with the level of care that is expected and required by the mission and the condition of the patient. Except as noted in Joint Publication 1 regarding exceptional circumstances, the advertised capability must be present during transport, or increased morbidity and mortality rates will result. This has been demonstrated across evidence-based medical reviews and studies.1 Many commanders of ERC programs are non-medically trained professionals (pilots, combat arms, etc.). Commanders should work in conjunction with assigned medical directors at the local, field, and theater level to ensure end unit continuity.
Health care teams are composed of a variety of different provider types, and the ERC mission is no exception. ERC providers must receive formal education and training to ensure platform familiarization and platform crew resource management. Updating military ERC systems based on cautious application of civilian best practices should be tempered by a realistic understanding of operational considerations. Over 67% of civilian Helicopter Emergency Medical Services (HEMS) agencies in the United States staff their helicopters with a Critical Care or Emergency Trauma Flight Nurse and Critical Care Flight Paramedic team.15 Most ground EMS agencies use some variation of an EMT, Paramedic, and Critical Care Nurse team. International HEMS agencies frequently use physician-led critical care transport teams.
The National EMS Scope of Practice Model is the core document that describes the scope of practice for civilian EMS providers in the United States.14 These civilian levels of EMS providers, typically applied to enlisted medical providers, are Emergency Medical Responder, EMT, Advanced EMT, or Paramedic. Registered Nurses (RN) with education and training applicable to prehospital care have several advanced certifications available to validate their skill and knowledge proficiency, including Certified Flight RN, Certified Transport RN, and others. Several international EMS systems educate, train, and certify physicians as prehospital providers. Some Emergency Medical Services Fellowship programs for physicians in the U.S. train physicians to provide care in the field, and others are more administrative functions of EMS Medical Direction.
The United Kingdom (UK) Medical Emergency Response Team platform is the most well-known for use in the Regional Command South of Afghanistan (c 2005-2020).
Higher competency and capability improve case fatality rates when patients are transported. During Operation Enduring Freedom, care provided by critical care flight paramedics showed a 66% lower risk of 48-hour mortality compared with that of basic level EMTs.16, 36 In the UK, prehospital critical care is provided by physician-staffed HEMS. These teams have demonstrated survival in cases previously thought to be non-survivable (e.g., traumatic cardiac arrest).17 British military platforms with on-board intensivists have likewise demonstrated improved survival in more severely injured patients. 18
It is imperative to understand the attributes of the different provider types based on their qualifications and certifications. Instrumental to ensuring capability is the verification of the currency of their practice experience and their skill proficiency. Additionally, well-trained teams improve outcomes, so ERC teams that train together prior to operational assignment may optimize patient outcomes.
Transport Platforms & Medical Materiel
Patient transport is conducted as a planned component of a given mission aboard dedicated platforms or transport of opportunity. Understanding the capabilities and limitations of the transport platform will help ERC providers, mission planners, and medical control optimize the care they deliver. This requires the appropriate selection capability to conduct the mission based on the provider team, resuscitative equipment, treatment protocols, and vehicular capabilities to move through the environment. For some ERC missions, the transport may require serial transfers between different platforms and modes of transport. All phases of transport must be considered by the ERC team to ensure they have the proper amount of consumables for the entire transport, such as oxygen. Familiarization with the different platforms available in a theater of operation is imperative.
When planning for LSCO, the frequency of multiple platforms and transfer legs between roles of care increases in relation to the combat environment. A single helicopter ride from Role 1 to Role 3 is likely not an option during this type of event. Multiple ground transport moves may be required prior to the utilization of an air asset.
Weight and space restrictions, as well as the challenges of patient transport in an operational setting, necessitate the deliberate and careful selection of medical materials for a given mission. The provider’s competency and the medical material actually present in the platform determine ERC capability. Platform selection will directly impact personnel and equipment availability and determine the highest level of care. Platforms should be chosen with an understanding of the patient's condition and must be appropriate for the type of ERC provider. Specific medical materials designated as patient movement items (PMI) must be available to support the patient during every phase of transport. Examples of PMI include ventilators, patient monitors, pulse oximeters, suction machines, IV pumps, oversized litters, negative pressure wound vacuums, pneumatic compression stockings/devices, etc.19 It is important that the transferring facility requests these items so that they can be loaded and transported with the ERC team. Whenever possible, the expendable medical supplies like oxygen from the transferring facility should be used until the last safe moment before departure. This action conserves the onboard medical supplies, which cannot be replenished without stopping and delaying the transport. Additional information on PMI is found in the AE Equipment Standards (AFI 10-2909), JP 4-02, and FM 4-02.1.20,21
Patient Movement/Evacuation Coordination Elements
Effective MEDEVAC and ERC rely on a dedicated coordination element possessing a comprehensive understanding of the operational environment, transportation networks, and asset capabilities. This element must integrate operational, clinical, and medical regulating functions across all military levels, ensuring casualties are moved at the right time, with the right care, to the right location.22 During Operation Freedom’s Sentinel, the Patient Evacuation Coordination Cell (PECC) successfully synchronized tactical medical evacuation efforts throughout Afghanistan. As the nerve center for MEDEVAC, the PECC validated requests, forecasted patient flow, and allocated ERC resources, ensuring patients received the right care, at the right time, and in the right place. For future success, a coordination center/cell requires clearly defined authorities, a joint structure, governing directives, and formal tasking relationships to manage intratheater patient evacuation. Empowered by the Combatant Commander, it must issue taskings, prioritize missions, and clinically manage ERC. Integration with command-and-control systems, logistics, and medical regulating structures, along with real-time situational awareness tools, is crucial for effective tasking and decision support. Without these authorities and mechanisms, synchronization across joint, interagency, and coalition environments are compromised.
Evacuation Requests: Point of Wounding, Illness, Injury
Two types of requests may occur in a theater of operation: the first is initiated when a 9-Line MEDEVAC Request is received from personnel at the point of wounding, illness, or injury. This is a standardized form used to communicate essential operational information to the coordination center/cell. While it contains Patient Precedence (Urgent, Urgent Surgical, Priority, Routine, Convenience), it lacks robust clinical information captured through a patient assessment and documented electronically (i.e., Battlefield Assisted Trauma Distributed Observation Kit [BATDOK] or on DoD Form 1380, Tactical Combat Casualty Card detailing a M.I.S.T. [Mechanism of Injury, Injuries, Signs & Symptoms and Treatments]). Report that supports clinical decision-making and intelligent tasking executed by the coordination center/cell to ensure casualties are operationally moved with the right ERC, at the right time, to the right location for the right care.
Movement Requests: Interfacility Transfers
9-Line MEDEVAC Requests can be used to request transfers between the Roles of Care but will require more clinical information to support the planning and coordination required to meet the needs of the patient and validate the level of ERC required to safely move high acuity patients, maintain clinical stability, and manage ongoing complex physiological needs in a dynamic transport environment. See Appendix A for the NATO 9-line MEDEVAC Request.
In addition to the 9-Line, patient movement requests can be submitted through the DoD information system called USTRANSCOM Regulating and Command & Control Evacuation System (TRAC2ES), (https://trac2es.transport.mil/) starting from Role 2, both surgical and non-surgical. Coordination centers/cells receive 9-Lines through the normal channels and use TRAC2ES as the system of record to plan, coordinate, and synchronize movement between roles of medical care, assign the right ERC team to execute, and conduct post-mission reviews for performance improvement and patient safety events.
No matter which system is used to coordinate movement, the senior medical person caring for the patient(s) determines movement precedence, timeline of when it will be safe to move, and is responsible for ensuring the patient(s) meet the clinical guidelines for ERC. The coordination center/cell is responsible for ensuring the right ERC team and platforms support the patient movement mission.
CAUTION: Terminology used to communicate precedence is not consistent across services. Terminology for air (rotary wing) and ground ambulances shall be used for inter-facility transport and is provided in Table 2.

Medical Direction
Medical direction is a critically important aspect of ensuring the delivery of an expected capability of care in the out-of-hospital environment.25-27 While medical direction may be delegated to any physician regardless of specialty, it does require unique knowledge and skills. Medical direction has traditionally been the responsibility of the unit physician (flight surgeon for example), although most of these providers do not receive additional formalized or structured education or training for this duty. Most flight surgeon training programs focus on pilot medical readiness and not critical care transport of sick and injured patients.
Medical direction encompasses both online and offline clinical guidance.25 This OPG defines medical direction as the direct technical authority to determine capability, promulgate medical policy, and most importantly, the authority to enforce the standard of care through quality assurance with local privileging (official designation of ability to perform medical mission, not necessarily the hospital version of “credentialing”) actions of individual ERC providers. Online medical direction includes both the on-scene medical supervision of providers actively engaged in patient care, as well as real-time clinical guidance of providers via telecommunication.28 Offline medical direction includes protocol development and review, continuing education of prehospital providers, quality improvement activities, and other duties designed to increase the quality of the system, but are not related to immediate and direct patient care.25 Medical direction can occur at many levels. This OPG will focus on the requirements and responsibilities for unit-level medical direction and regional medical direction. The primary mission of the medical director is to ensure that the commander is effectively advised on the technical requirements of MEDEVAC, and the transport unit is providing the expected patient care capability and quality.
The commander of the unit assigned to perform MEDEVAC should appoint the unit’s physician as the medical director. The medical director is responsible for the technical control and supervision of all en route medical activities of the command and the commander delegates that authority in writing. This additional duty order should also include the authority to privilege ERC providers within that organization. It should also include delegation of the authority and prerogative to hold in abeyance, to deny, or to immediately but temporarily suspend clinical privileges/practice when there is reasonable cause to doubt the individual’s competence to practice or for any other cause affecting the safety of patients or others. The specific intent of the medical director’s decision to implement temporary adverse privileging actions should be the safety and well-being of all patients and safeguarding the quality and efficiency of care delivered by the ERC organization. If a unit physician is not available to provide medical direction, the unit conducting MEDEVAC should coordinate with the supporting MTF for a shared medical director.
Minimum Qualifications for Unit Medical Director
- Duly commissioned officer in the Medical Corps of the Armed Forces of the United States.
- Knowledge of the ERC mission provided by the unit, unit treatment protocols and CPGs, and capabilities of the unit's providers.
- Completion of the Tactical Combat Medical Care or similar course.
- Completion of the Joint En Route Care Course or similar course.
- Medical director and operational medicine training.
Desirable Qualifications for Unit Medical Director
- A physician who has attended an EMS Fellowship and is EMS Board certified, as recognized by the American Board of Medical Specialties.
- Board certification or eligibility in any specialty recognized by the American Board of Medical Specialties or the American Osteopathic Association (ideally Emergency Medicine, Anesthesia, General Surgery, or Critical Care), or experience in operational medicine.
- Experience in medical direction for ERC.
Unit Medical Director Responsibilities
Offline medical direction:
- Chart reviews of all cases are personally or through delegation.
- Continuous quality assurance/performance improvement activities.
- Detailed case reviews on selected cases from chart review protocol variations or high-risk low-frequency interventions.
- Oversight of education and training of unit medical providers.
- Notify the next higher level of command surgeon/theater medical director of systemic issues identified.
- Conduct a quality assurance program and performance improvement program to ensure standardization of care delivered in accordance with regulations or instructions and Service and Combatant Command policies, while validating practices, and propose new practices in ERC.
- Unit privileging, through technical oversight and supervision, ensuring that providers are trained, qualified, current, and proficient in their ERC duties and responsibilities.
- Ensures completion and delivery of patient care reports into the patient record and the JTS.
Online medical direction:
Due to communication and patient care challenges unique to the deployed environment, online medical direction may be most effectively done by physicians other than the transporting unit medical director.29
Priority of online medical direction is:
- Transferring physician.
- Receiving physician.
- Transporting unit medical director.
The transporting unit medical director is responsible for ensuring providers know who and under what circumstances to call for online medical direction. It is important to plan/discuss whenever possible any anticipated scenarios requiring deviation from established ERC provider protocols with the transferring physician to ensure required medical supplies are available during transport.
Medical direction is required at the unit level and at the regional level (PECC). Medical direction at the regional level is centered on offline medical direction activities. Regional medical director works continuously to increase the quality of care delivered during intra-theater transport. Regional medical direction may occur at different levels based on the operating environment but will typically be at the level of the joint operations area and lower. The Joint Force Surgeon’s office is the doctrinal proponent for intra-theater patient transport and should assign regional medical directors. A best practice is to appoint a consultant at the Combined Joint Task Force level for EMS and ERC. The Joint Force Surgeon’s office shall provide regional medical direction unless they delegate this authority to subordinate regional medical directors.
Minimum Qualifications for Regional Medical Director
- Board Certification in a specialty recognized by the American Board of Medical Specialties or the American Osteopathic Association, and experience in operational medicine and/or extensive experience in ERC.
- Knowledge about the transporting environment and capabilities of units operating in theater.
Regional Medical Director Responsibilities
- In conjunction with medical planners, advise the Combatant/Theater Commander on the medical common operating picture and allocation of resources for intra-theater transport.
- Ensure the requirements of documentation of intra-theater transport care are met.
- Assist medical directors operating in theater and ensure they have the knowledge and skills to perform the job.
- Provide technical supervision to medical directors in theater.
- Ensure relevant out-of-hospital research is supported and accomplished.
- Ensure information from intra-theater transportation is supplied to the DoD Trauma Registry.
- Regional protocol development
The JTS CoERCCC recommends the development of service-agnostic courses for Medical Corps officers to serve as entry-level training for medical directors covering the fundamentals for physician leadership in EMS and ERC oversight and direction. ERC experienced Nurse Practitioners or Physician Assistants may serve as local medical directors under a Regional Medical Director who is a licensed and board-certified physician.
Treatment Protocols
Recognition of the value of hospital-based CPGs led the Institute of Medicine in 2006 to recommend an evidence-based model for prehospital care protocols addressing treatment, triage, and transport.29 These protocols standardize care, reduce errors, and ensure appropriate treatment, particularly for non-physician providers who must often make decisions without direct physician input. Widely used in civilian EMS and in the U.S. Army’s Critical Care Flight Paramedic program, protocols guide practice within providers’ limited scope.
Evidence supports their effectiveness: a systematic review in the Netherlands showed significant improvements in care processes and modest outcome gains, an Intensive Care Unit (ICU) study reported reduced mortality after protocol adoption, and a prehospital study found protocol-based guidance slightly improved decision-making and decreased scene times compared with online medical direction.30-32 While system-level research remains limited, numerous individual protocol studies show improved outcomes.33,34
Beyond guiding care, protocols enable quality assurance and research by standardizing practice, identifying deviations, and addressing gaps.35 They require regular review, at least annually, and should be developed regionally by medical directors and adapted locally with regional approval.35,36
Documentation of Care
Inter-facility patient transport must be documented on an approved patient care record (PCR). JTS-approved PCRs include:
- DD Form 1380 TCCC Card
- DA Form 4700 (JTS Approved 20251105)
- AF IMT 3899 Patient Movement Record (20060819, V1)
- Medical Rescue Report SAR Form 3-50.1A
- BATDOK when fully approved and operational
The DA Form 4700 is primarily used for rotary wing transport from POI or inter-facility transfer. The AF IMT 3899 is primarily used for AE, with supplements A through K as indicated for Critical Care Air Transport Team movements. The Rescue Report SAR Form 3-50.1/1 contained within NTTP 3-50.1, Navy Search and Rescue Manual, is required whenever a search or rescue is attempted or accomplished that involves Navy personnel or assets. Completed Rescue Reports must be submitted to the Navy Chief of Naval Operations Search and Rescue Model Manager’s office.
When completing the PCR, ensure the patient’s name on the PCR matches the name entered on arrival to the MTF. In cases where a casualty’s name is unknown, the MTF will utilize theater-predetermined trauma identities. Transport teams must obtain an ID sticker at the time of handover to the MTF to ensure the correct identity is recorded on the PCR.
The PCR should be completed and delivered to the receiving MTF along with the patient. Completed PCRs and After Action Reviews should be encrypted and submitted to JTS Patient Evacuation at the following email address: dha.jbsa.healthcare-ops.list.jts-patient-evacuationl@health.mil. If unable to encrypt, documentation may be sent encrypted utilizing DoD Secure Access File Exchange. A follow-up email with the “Passphrase” for encryption will have to be sent separately to the JTS Patient Evacuation email to allow for download of the file(s).
Patient Transport Criteria

References
- Walrath B. Searching for systems-based solutions to enhance readiness. Navy Medicine Live online blog.
- Shackelford SA, Remley MA, Keenan S, Kotwal RS, Baker JB, Gurney J, Rush S, Friedrichs P. Evidence-based principles of time, triage and treatment: Refining the initial medical response to massive casualty incidents. J Trauma Acute Care Surg. 2022 Aug 1;93(2S Suppl 1): S160-S164.
- Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001–2011): implications for the future of combat casualty care. Journal of trauma and acute care surgery, Dec 2012. 73(6), S431-S437.
- National Highway Traffic Safety Administration. Guide for interfacility patient transfer. Apr 2006. https://www.ems.gov/assets/Interfacility_Transfers.pdf Accessed Dec 10, 2025
- Warren J, Fromm RE Jr, Orr RA, Rotello LC, Horst HM; American College of Critical Care Medicine. Guidelines for the inter- and intrahospital transport of critically ill patients. Crit Care Med. 2004 Jan;32(1):256-62
- Dunn MJ, Gwinnutt CL, Gray AJ. Critical care in the emergency department: patient transfer. Emergency Medicine Journal, Jan 24, 2007, 40-44.
- Gray A, Bush S, Whiteley S. Secondary transport of the critically ill and injured adult. Emergency Medicine Journal, 2004. 21, 281-285.
- Whiteley S, Macartney I, Mark J, Barratt H, Binks R. Guidelines for the transport of the critically ill adult. Intensive Care Society. 3rd edition, 2011.
- Blow O, Magliore L, Claridge, et al. The golden hour and the silver day: detection and correction of occult hypoperfusion within 24 hours improves outcome from major trauma. Journal of Trauma, Nov 1999. 47, 5, 964-969.
- Meregalli A, Oliveira RP, Friedman G. Occult hypoperfusion is associated with increased mortality in hemodynamically stable, high-risk, surgical patients. Critical Care, 8, 2, 2004. R60-R65.
- Thom O, Taylor DM, Wolfe RE, Myles P, Krum H, Wolfe R. Pilot study of the prevalence, outcomes and detection of occult hypoperfusion in trauma patients. Emerg Med J. 2010 Jun;27(6):470-2.
- Raum M, Rixen D, Linker R, Gregor S, Holzgraefe B, Neugebauer E. Beeinflussung der Plasma-Laktatkonzentration durch laktathaltige Infusionslösungen [Influence of lactate infusion solutions on the plasma lactate concentration]. Anasthesiol Intensivmed Notfallmed Schmerzther. 2002 Jun;37(6):356-8. German.
- Association of Critical Care Transport. The Critical Care Transport Standards Project Version 3. 20
- National Association of State EMS Officials. National EMS Scope of Practice Model 2019: Including Change Notices 1.0 and 2.0. 2021-08-01. https://rosap.ntl.bts.gov/view/dot/56917
- Cone D, Brice JH, Delbridge TR, et al. Emergency Medical Services: Clinical Practice and Systems Oversight, 2 Vol Feb 2015. John Wiley & Sons. ISBN: 978-1-118-86530-9.
- Apodaca A, Olson Jr CM, Bailey J, et al. Performance improvement evaluation of forward aeromedical evacuation platforms in Operation Enduring Freedom. Journal of trauma and acute care surgery, 2013. 75(2), S157-S163.
- Davies GE, Lockey DJ. Thirteen survivors of prehospital thoracotomy for penetrating trauma: a prehospital physician-performed resuscitation procedure that can yield good results. Journal of Trauma and Acute Care Surgery, May 2011. 70(5), E75-E78.
- Kehoe A, Jones A, Marcus S, et al. Current controversies in military pre-hospital critical care. Journal of the Royal Army Medical Corps, 2011. 157 (Suppl 3), S305-S309.
- S. Department of the Air Force. Aeromedical Evacuation Equipment Standards (AFI10-2909). Jul 23, 2013.
- Joint Health Services, Joint Publication 4-02. Dec 11, 2017.
- Department of the Army. Army Techniques Publication 4‑2: Medical Evacuation. U.S. Army Training and Doctrine Command; 2019.
- Headquarters Department of the Army. Casualty Evacuation. Army Techniques Publication No. 4-02.13, Jun 30, 2021.
- Headquarters Department of the Army. Army Health System Support to Maneuver Forces (ATP 4-02.3) Army Techniques Publication No. 4-02.3 Jun 2014.
- S. Air Force. En Route Care and Aeromedical Evacuation Medical Operations (AFI 48-107). Dec 15, 2020.
- Alonso-Serra H, Blanton D, O'Connor RE. Physician medical direction in EMS. Prehospital Emergency Care, 1998. 2(2), 153-157.
- Delbridge TR, Bailey B, Chew J, et al. EMS agenda for the future: where we are… where we want to be. Annals of emergency medicine, 1998. 31(2), 251-263.
- American College of Emergency Physicians. Interfacility transportation of the critical care patient and its medical direction. Annals of Emergency Medicine, 2006. 47(3), 305.
- Wuer, RC, Swope GE, Holliman CJ, Miguel GVD. On-line medical direction: a prospective study. Prehospital and disaster medicine, 1995. 10(03), 174-177.
- Institute of Medicine Committee on the Future of Emergency Care in the US Health System. Emergency medical services: at the crossroads. 2007. Washington: DC.
- Lugtenberg M, Burgers JS, Westert GP. Effects of evidence-based clinical practice guidelines on quality of care: a systematic review. Quality and Safety in Health Care, 2009. 18(5), 385-392.
- Afessa B, Gajic O, Keegan MT, et al. Impact of introducing multiple evidence-based clinical practice protocols in a medical intensive care unit: a retrospective cohort study. BMC emergency medicine, 2007. 7(1), 1.
- Rottman SJ, Schriger DL, Charlop G, et al. On-line medical control versus protocol-based prehospital care. Annals of Emergency Medicine, 1997. 30(1), 62-68.
- Jones AE, Focht A, Horton JM, Kline JA. Prospective external validation of the clinical effectiveness of an emergency department-based early goal-directed therapy protocol for severe sepsis and septic shock. CHEST Journal, 2007. 132(2), 425-432.
- McFadden ER, Elsanadi N, Dixon L, et al. Protocol therapy for acute asthma: therapeutic benefits and cost savings. The American Journal of Medicine, 1995. 99(6), 651-661.
- Pines JM, Fee C, Fermann GJ, et al. The role of the society for academic emergency medicine in the development of guidelines and performance measures. Academic Emergency Medicine, 2010. 17(11), e130-e140.
- Mabry RL, Apodaca A; Penrod J, et al. Impact of critical care–trained flight paramedics on casualty survival during helicopter evacuation in the current war in Afghanistan. Journal of Trauma and Acute Care Surgery 2012. 73(2), S32–S37
Appendix A: 9-Line MEDEVAC Request

Download in PDF
READ FULL PDF
READ FULL PDF
READ FULL PDF
READ FULL PDF